Download
1 / 35
710 likes | 2.13k Views
Peripheral Arterial Disease (PAD). M. Saifur Rohman , dr SpJP . PhD. FICA Dept of Cardiology and Vascular Medicine Faculty of Medicine, Brawijaya University. Overview. PAD (peripheral arterial disease) – a marker for MI and IS Epidemiological data on PAD Risk factors Prevalence

E N D
Peripheral Arterial Disease(PAD) M. SaifurRohman, drSpJP. PhD. FICA Dept of Cardiology and Vascular Medicine Faculty of Medicine, Brawijaya University
Overview • PAD (peripheral arterial disease) – a marker for MI and IS • Epidemiological data on PAD • Risk factors • Prevalence • Atherothrombosis – coexistence of PAD, coronary and cerebrovascular disease • Natural history • Low ABPI as an independent predictor of ischaemic risk • Symptomatology of PAD • Diagnosis and management of PAD • Clopidogrel – a new standard of treatment for atherothrombosis
PAD – a marker for MI and IS • Atherothrombosis = thrombus formation on top of existing atherosclerosis • Occurs in multiple arterial beds Cerebrovascular disease (ischaemic stroke, transient ischaemic attack) Coronary artery disease (stable/unstable angina, myocardial infarction) PAD (intermittent claudication, critical leg ischaemia, amputation, gangrene, necrosis)
Risk factors for PAD • Gender (male) • Age • Smoking • Hypertension • Diabetes • Hyperlipidaemia • Fibrinogen • Homocysteinaemia PAD Atherosclerosis Atherothrombosis Ischaemic stroke Myocardial infarction Murabito JM et al. Circulation 1997;96:44–49; Laurila A et al. Arterioscler Throm Vasc Biol 1997;17:2910–2913;Malinow MR et al. Circulation 1989;79:1180–1188; Brigden ML. Postgrad Med 1997;101:249–262.
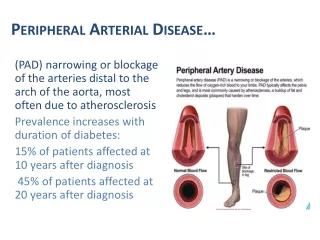
Prevalence of PAD – variation according to diagnostic criterion • 6.3 million individuals with symptomatic, established PAD are diagnosed in the USA and EU1 • Epidemiological studies imply that real* prevalence may be approx. 20 million (= 9.5% of the population > 50 years old) • In 613 men and women (mean age 66 years), real prevalencewas found to be underestimated by two- to seven-fold2 • ABPI (ankle:brachial pressure index) correlates with angiographically determined disease3 • ABPI < 0.9 is a marker of diffuse atherothrombosis4 1 17 Western European countries. Statistical Supplement; WHO Yearbooks, Annual Statistics, 1997; 2 Criqui MH et al. Vasc Med 1997;2:221–226; 3Shinozaki T et al. J Clin Epidemiol 1998;15:1263–1269; 4Kornitzer M et al. Angiology 1995;46:211–219. *ABPI < 0.9, symptomatic or not, diagnosed or not.
Epidemiology of PAD – effect of age and gender • Epidemiological data on PAD vary according to: • Population studied • Method of diagnosing PAD • Incidence and prevalence of intermittent claudication* increase with age • Prevalence in men aged 45–50 years is 1% • Prevalence is 3–3.5% in men aged > 50 years • Similar trend in women, increase with age • More common in men than in women • Twice as many men as women aged > 50 years have intermittentclaudication (3.5% and 2%, respectively) • Predominance in males disappears after age of 70 Weitz JI et al. Circulation 1996;94:3026–3049. * Rose questionnaire criteria Bull. Wld Hlth Org. 1962;27:645-658
Atherothrombosis – coexistence of symptomatic PAD and coronary or cerebrovascular disease 50 Men Women 40 Concurrent cardiovascular disease (MI, CABG, stroke or stroke surgery) 30 Percentage of group 20 10 0 Yes No Yes No PAD Criqui MH et al. Vasc Med 1997;2:221–226.
Atherothrombosis – symptomatic atherosclerosisin CAPRIE(overlap between PAD, CAD and CVD) CAPRIE1(n = 19185) Cerebrovascular disease (CVD) Coronary artery disease (CAD) 7.3% 29.9% 24.6% 3.3% 11.9% 3.8% 19.2% Peripheral Arterial Disease (PAD) 1CAPRIE Steering Committee. Lancet 1996;348:1329–1339.
5-year natural history of PAD 100 patientswith claudication who do notseek medical advice 100 patients with asymptomatic PAD 100 patients diagnosedwith claudication Local Events Systemic Events Worsening claudication25 patients 10 to 20 non-fatal MIs or strokes PLUS Surgical revascularization 10 patients 30 deaths: • CHD 15 • Other cardiovascular and cerebrovascular 5 • Non-cardiovascular 10 Major amputation 2 patients Dormandy JA. Hosp Update 1991;April:314–318.
PAD mortality – 10-year survival rates of subjects in the San Diego Artery Study 1.00 Normal 0.75 Asymptomatic Survival 0.50 Symptomatic 0.25 Severe symptomatic 0.00 0 2 4 6 8 10 12 Time (years) Criqui MH et al. N Engl J Med 1992;326:381–386.
Intermittent claudication – an independent risk factor for increased mortality rates • In the Whitehall study (n = 18 388), mortality rates in individuals with intermittent claudication were twiceas high as those in healthy controls (17 years’ follow-up study) • Increased mortality even after adjustment for coronary risk factors • Cardiac ischaemia at baseline • Systolic blood pressure • Plasma cholesterol concentration • Smoking behaviour • Employment grade • Degree of glucose intolerance Smith GD et al. Circulation 1990;82:1925–1931.
Low ABPI is a strong predictor ofcardiovascular mortality • Reduced ABPI is a significant independent predictor of cardiovascular and coronary mortality • Age-adjusted relative risks for 10-year cardiovascular and coronary mortality are higher in those with ABPI < 0.9 • The risk of cardiovascular death increases with decreasing ABPI • ABPI measurement is underutilized and can be usefully incorporated in risk assessment and screening programmes • ABPI measurements are inexpensive, simple and non-invasive Kornitzer M et al. Angiology 1995;46:211–219. McKenna M et al. Atherosclerosis 1991;87:119–128. Dormandy JA et al. J Cardiovasc Surg 1989;30:50–57.
2.5 2.0 1.5 1.0 0.0 0.2 0.4 0.6 0.8 1.0 ABPI ABPI – inverse relationship with 5-year risk of cardiovascular events and death 10.2% relative risk increaseper 0.1 decrease in ABPI (p = 0.041) Risk relative to ABPI Dormandy JA, Creager MA. Cerebrovasc Dis 1999;9(Suppl 1):1–128 (Abstr 4).
Symptomatology of PAD • Intermittent claudication • Exercise-induced ischaemic calf-muscle pain while walkingand/or weakness, relieved by rest • Mortality rate from stroke and MI two to three times greaterthan in age-matched controls1 • Prognosis varies with multiple risk factors and/or severityof disease • Critical limb ischaemia • Pain at rest, eventually resulting in gangrene and amputation2 1Dormandy JA et al. J Cardiovasc Surg 1989;30:50–57. 2European Working Group on Critical Leg Ischemia. Circulation 1991;84(Suppl IV):IV1–IV26.
Diagnosis of PAD • Evaluation of pulses and auscultation of bruits • Ankle:arm blood pressure index (ABPI) • Ratio of ankle:brachial systolic blood pressure • Simple, non-invasive, suitable for routine screening • Exercise testing • Pain-free and maximal walking distance • Size and duration of drop in ankle systolic BP upon claudication Weitz JI et al. Circulation 1996;94:3026–3049.
Thrombus formation Acute Limb Ischemia Thrombus forms and extends into the lumen Thrombus Lipid core Adventitia Weissberg, 1999
Definition of Acute Limb Ischemia Sudden decrease of arterial limb perfusion causing threat to limb viability
Etiology of acute limb ischemia Acute arterial embolism: Of a relatively health arterial tree Acute arterial thrombosis: Of a previously diseased arterial tree Acute traumatic ischemia:
Acute Thrombotic Ischemia Atherosclerosis causes progressive narrowing of the arterial tree Stimulates development of collaterals Acute Embolic Ischemia Pathophysiology An embolus suddenly occludes a relatively healthy arterial tree It usually arrest at arterial bifurcation Sluggish flow & rough surface will favor acute thrombosis Aortic bifurcation Iliac bifurcation Femoral bifurcation Popliteal trifurcation An embolus can originate from the heart(MS with atrial fibrillation, MI with mural thrombus) or dilated diseased arteries(aortic aneurism)
It is important to differentiate between embolic & thrombotic ischemia: Because the management is different • Clinical Features Suggestive of acute Embolism: • Sudden onset of symptoms • Known embolic source • Absence of previous claudication • Normal pulse in the other limb
One axial a. with limited collateral pathways Aorta & common iliac Two axial aa. With better collateral potentials Internal & external iliac Two axial aa. With better collateral potentials Superficial & deep femoral Popliteal artery One axial a. with limited collateral pathways Tibial arteries Three axial aa. with better collateral potentials The severity of acute ischemia depends on: a) Capability of existing collaterals to carry blood around the acute obstruction (collaterals are more developed in patients with preexisting chronic ischemia) Accordingly, arterial embolism is more likely to produce sudden symptoms & severe ischemia then arterial thrombosis b) The location of obstruction in relation to the number of axial arteries c) The extent of obstruction The larger the obstruction, the more collaterals are lost d) The duration Flow distal to the obstruction is sluggish. If collaterals cannot increase the flow above a critical point, a stagnation clot will develop in the distal arterial tee. This the reason why heparin should be given as early as possible For Example: Popliteal a occlusion (a single axial a.) results in severe ischemia, while posterior tibial occlusion may be asymptomatic if other leg arteries are patent
Clinical Evaluation of Acute Ischemia (Clinical Picture) Symptoms of acute ischemia: Pain: Diffuse foot & leg severe aching pain of acute onset (more acute in embolic ischemia) Pain may diminish in intensity by time if collaterals open improving circulation, or if ischemia progresses causing ischemic sensory loss Coldness is an early symptom Numbness followed by sensory loss (late) Muscle weakness (heavy limb) followed by paralysis (late)
Clinical Evaluation of Acute Ischemia (Clinical Picture) Inspection COLOR: Early: pale Later: cyanosed mottling fixed mottling & cyanosis Fixed mottling & cyanosis An area of fixed cyanosis surrounded by reversible mottling Pallor Reversible mottling Signs of acute ischemia 5Ps Pain: symptom + Pale Pulseless Parathesia Empty veins: compare the Rt. (ischemic) & Lt. (normal) Paralysis
Clinical Evaluation of Acute Ischemia (Clinical Picture) Light touch Vibration sense Proprioreception Deep pain Pressure sense Late Signs of acute ischemia Palpation 5Ps Loss of sensory function Numbness will progress to anesthesia Pain: symptom + Progress of Sensory loss Pale Pulseless Parathesia Paralysis
Clinical Evaluation of Acute Ischemia (Clinical Picture) Signs of acute ischemia Palpation 5Ps Loss of motor function: Indicates advanced limb threatening ischemia Pain: symptom + Late irreversible ischemia: Muscle turgidity Pale • Intrinsic foot muscles are affected first, followed by the leg muscles • Detecting early muscle weakness is difficult because toes movements are produced mainly by leg muscles Pulseless Parathesia Paralysis
Summary • PAD is a marker of atherosclerosis in the coronary and cerebral arteries • PAD is often underestimated and underdiagnosed, and requires proper diagnosis: • Risk factors need to be managed: smoking cessation, regular exercise training • Atherogenesis=CAD • Plaque rupture=Limb Ischemix

![Diffuse Vascular Disease (Focus on Peripheral Arterial Disease [PAD])](https://cdn1.slideserve.com/3363465/slide1-dt.jpg)