Download
1 / 20
240 likes | 349 Views
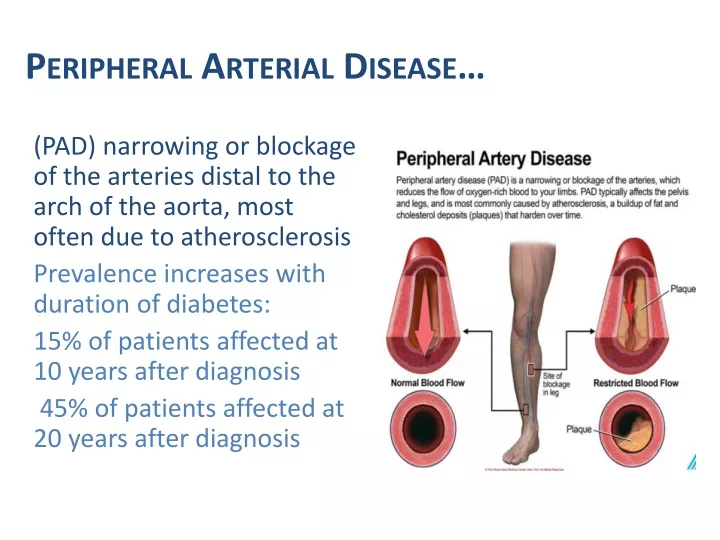
Peripheral Arterial Disease…. (PAD) narrowing or blockage of the arteries distal to the arch of the aorta, most often due to atherosclerosis Prevalence increases with duration of diabetes: 15% of patients affected at 10 years after diagnosis

E N D
Peripheral Arterial Disease… (PAD) narrowing or blockage of the arteries distal to the arch of the aorta, most often due to atherosclerosis Prevalence increases with duration of diabetes: 15% of patients affected at 10 years after diagnosis 45% of patients affected at 20 years after diagnosis
Clinical Features of PAD… Reduced/Absent foot pulses Skin - thin, shiny and without hair Colour - may be a dusky red (due to stagnation of blood in maximally dilated arterioles), pale and mottled or cyanotic blue Temperature - skin feels cool or cold to touch Loss of fat padding over bony prominences Patient may complain of intermittent claudication (though neuropathy can render the most severe IC painless) Rest Pain – worse at night – dangling legs out of bed for relief
People without Diabetes Peripheral Arterial Disease People with Diabetes Earlier onset and more prevalent Affects the more distal vessels (below knee) More severe and diffuse Often asymptomatic – or atypical ABPI can be unreliable Media calcinosis (Monckeberg’s sclerosis) Later age/lifestyle related onset Affects mainly proximal vessels More localised lesions Intermittent claudication pain Less likely to cause thrombus formation ABPI reliable Other risk factors include age, smoking, hypertension and hyperlipidemia plus peripheral neuropathy in diabetes Inverse relationship between PAD and alcohol consumption
Comparing feet is useful! PAD often worse on one side
Other Risk Factors Neuropathy and PAD are the big risk factors, but there are other risk factors for developing foot problems
structural abnormality of the foot “A change in foot shape that results in a difficulty in fitting shoes which could be purchased in high street shops” (Scottish Diabetes Group – Foot Action Group 2010).
Skin Changes Significant Callus Callus on a weight bearing area increases the risk of ulceration by approx 77 times 80% chance of ulceration if blood stained callus
Mechanism of Callus Breakdown Disclaimer – podiatrists do not and cannot cause ulcers – we just find them!
Previous Ulceration is the highest risk factor for future ulceration After ulceration the affected area never repairs itself completely and only returns to 70% of tensile strength. This area is always vulnerable to future ulcerations, particularly when specialist footwear is not worn!
Inability to self care The inability for somebody to self care or the need to have help to self care can increase their risk of developing a foot problem Contributing Factors:
CKD & Diabetic Foot = HIGH risk Most people with end-stage renal failure & diabetes will have neuropathy Diabetes and renal disease both contribute to higher prevalence of pad Uraemia compromises defence against infection = Increased number of foot ulcers will be infected on first presentation Greater proportion will have osteomyelitis Anaemia = Poor tissue oxygenation and impaired wound healing Dialysis predicts foot ulceration independently of neuropathy & pad: Reduced ability to perform self-care/foot inspection Reduced visual acuity/Retinopathy Reduced mobility and manual dexterity Reluctance to attend other appointments
Footwear…(or lack of it!) Ill-fitting shoes and walking barefoot with insensitive feet are the most frequent cause of ulceration Regular footwear assessment is essential Individual advice on appropriate footwear for each patient essential Chronic oedema and bandaging often have causes problems in finding appropriate footwear Therapeutic footwear can have a beneficial effect in the primary and secondary prevention of diabetic foot ulceration Referral to an orthotist for footwear advice/supply should be considered if unable to fit into high street shoe
so we know what the foot problems are…(ulceration, infection, charcot) and what causes them…(Neuropathy, PAD, Deformity, Callus, Trauma) The challenge is… How do we prevent them???
Targeted preventive services can identify those at risk of ulceration and improve outcomes, and rapid access to multi-disciplinary foot care can lead to faster healing, fewer amputations and improved survivalNHS Diabetes 2012 WE LOOK FOR THEM!!!...…Diabetes Foot Screening ‘Diabetic foot screening is effective in identifying the level of risk of developing foot ulceration’ (SIGN 2010)
For adults with diabetes, assess their risk of developing a diabetic foot problem at the following times: When diabetes is diagnosed, and at least annually thereafter If any foot problems arise On any admission to hospital, and if there is any change in their status while they are in hospital NICE NG19 - 2015 Diabetic foot problems: prevention and management How often do we screen?
NICE 2015 Recommends: Assessing the risk of developing a diabetic foot problem When examining the feet of a person with diabetes, remove their shoes, socks, bandages and dressings, and examine both feet for evidence of the following risk factors: Neuropathy Deformity Limb ischaemia Infection/Inflammation Ulceration Gangrene Callus Charcot arthropathy
foot screening training • Planned for Practice nurses in City CCG • Awaiting further info from Practice Nurse Lead • Hopefully start May 2017 – PLT Sessions • Dates will be sent to GP practices once arranged
what do we do after screening? It all depends on what you find!
Low Risk Normal Sensation Palpable Pulses No risk factors (except callus alone) Annual foot assessment by trained health care professional Emphasise importance of foot care = Written and Verbal Education Refer to Podiatry only if Podiatric need Advise could progress to moderate/high risk