Download
1 / 20
200 likes | 425 Views
PERIPHERAL OCCLUSIVE ARTERIAL DISEASE. GEMP I Centre for Health Science Education Station 2. Acknowledgements : Some of the images have been taken from the following sources. Surgical Tutor, U.K. National Amputee Centre, Canada American Family Physician

E N D
PERIPHERAL OCCLUSIVE ARTERIAL DISEASE GEMP I Centre for Health Science Education Station 2
Acknowledgements: Some of the images have been taken from the following sources • Surgical Tutor, U.K. • National Amputee Centre, Canada • American Family Physician • University of Pittsburg Medical School • John Byrne, Albany Medical Centre, New York, USA • University of Maryland Medical school, U.S. • The Faculty of Health Sciences, University of the Witwatersrand, wishes to express their gratitude for the use of these images for a Third Year class in Clinical Skills
Station Learning Objectives • Recognise the presentation of chronic versus acute arterial occlusive disease • Recognise the signs and symptoms of critical ischaemia • Know the commonest causes of arterial occlusive disease • Have an understanding of the indications for amputation.
Arterial occlusive diseases Includes: • peripheral arterial occlusive disease • coronary artery disease, • cerebrovascular disease and
P.A.D. Acute vs. Chronic Occlusion • Sudden Onset: pain followed by parasthesiae and then loss of function. • Usually due to an embolus- Usually at sites of vessel bifurcation, or • A thrombus clot is already present in a diseased vessel • Gradual Onset: Long standing symptoms of intermittent claudication • In atheromatous vessels which were previously patent, A collateral circulation will have been present.
B Femoral Vein, adherent thrombus
Chronic arterial occlusion A Arterial thrombus in coronary Artery: courtesy Univ. of Pittsburgh
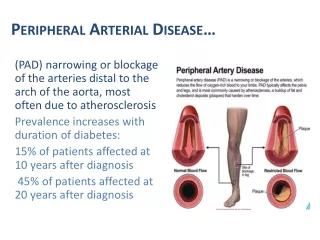
Risk Factors for P.A.D.(same as for atherosclerosis) • Diabetes Mellitus • Chronic Smokers • Hyperlipidaemia • Family history Note: Obesity also predisposes to atherosclerosis
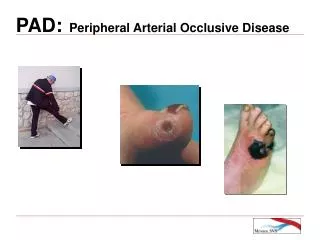
Features of P.A.D. Common Presenting symptoms: • Intermittent Claudication- a deep seated aching pain in the calves brought on by exercise, relieved by rest is an early symptom • Parasthesia • Rest Pain (late symptom) • Gangrene and Ulceration (late symptom) Features ofAcute occlusioninclude: • Pain • Pallor • Parasthesiae / numbness • Paralysis / weakness
On Examination you may expect to find • arterial bruits, • decreased or absent peripheral pulses, • decreased skin temperature, • dependent rubor, • dystrophic nails and shiny, hairless skin • gangrene • Ulceration See which of these features you are able to identify in the pictures in the following slide?
A B C E D
Claudication Distance(An indication of severity) Fontaine Stage Classification of PAOD • Stage I Asymptomatic, decreased pulses, ABI < 0.9 • Stage II Intermittent claudication • Stage III Daily rest pain • Stage IV Focal tissue necrosis PAOD = peripheral arterial occlusive disease; ABI = ankle-brachial index Grading Claudication • Initial Claudication Distance • Distance patient first experiences exertional pain • Absolute Claudication Distance • Furthest distance patient is able to walk Acknowledgenents: A.A.F.P.
The ankle-brachial index • Measures the ratio of lower to upper extremity blood pressure, • Is a significant predictor of cardiac events.
Principles of Treatment • Risk factor Modification • Anti-platelet agents • Exercise programme • Surgical Revascularisation • Bypass Methods • Amputation
InvestigationsANGIOGRAPHYMRI Arterial thrombus arch of Aorta Transfemoral Angiogram with Saphenofemoral Occlusion
Amputation • A properly performedamputationcan be: • Lifesaving for the patient, • May often be a better therapeutic alternative than an ill-conceived, futile attempt at a vascular reconstruction doomed to fail for lack of adequate recipient vessels. Major goalsof amputation surgery : • Preservation of functional length • Durable coverage • Preservation of useful sensation • Prevention of symptomatic neuromas • Prevention of adjacent joint contractures • Controlled short-term morbidity • Early prosthetic fitting, when applicable • Early patient rehabilitation
Assessment of amputation level in ischaemic lower limbs. • Currently there are no consistent criteria that can be applied before surgery. • The main objective of amputation is removal of sufficient diseased, infected and gangrenous tissue to permit the stump to heal but at the same time retain adequate limb length for prosthetic fitting“ • The use of a scoring system dependent on the preoperative angiogram to assess the run-off vessel situation provides a practicable and direct way to help predict the level of amputation in an ischaemic lower extremity. However, it is not totally reliable and should be used as one of the factors to be considered when an amputation is required. • Other invasive and non invasive techniques can also be utilised in assessment of circulation in determining amputation level pre-operatively • Assessment during the operation of local circulation is of extreme importance
Above knee amputation stump