Download
1 / 21
230 likes | 2.76k Views
Ambiguous Genitalia Neonatal Presentation. Baby H Born 11/08/2003 Mother - Somalian origin P4 G4 – others healthy, normal Booked, Rh negative, Syphilis negative, HIV negative Term, appropriate for gestational age, weight – 3322g Apgars – 8, 8, 9 Sent to nursery – unsure of sex

E N D
Ambiguous Genitalia Neonatal Presentation
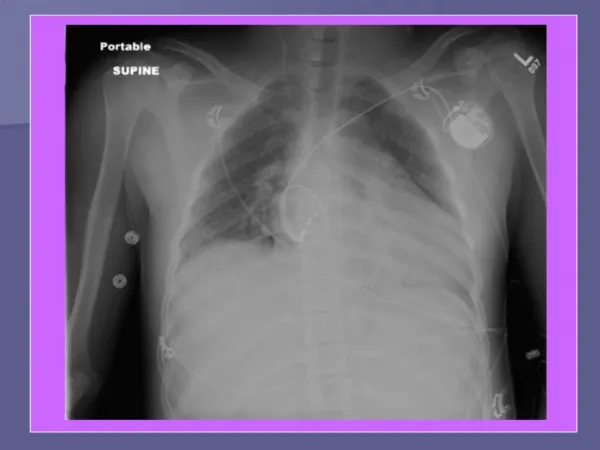
Baby H • Born 11/08/2003 • Mother - • Somalian origin • P4 G4 – others healthy, normal • Booked, Rh negative, Syphilis negative, HIV negative • Term, appropriate for gestational age, weight – 3322g • Apgars – 8, 8, 9 • Sent to nursery – unsure of sex • On examination – • Not dysmorphic • Blood pressure – 57/28 mmHg • Dextrostix – normal • Cardiac examination – 3/6 ejection systolic murmur, left sternal border • Genitalia – labioscrotal folds (unfused), palpable gonads, 1cm phallus, perineoscrotal hypospadias • Management and Progress • Stayed 1 week • Dextrostix normal, BP stable • Fed well
Day 3 – no urine output, distended bladder, required catheterisation - catheter fed into perineal opening • Passed urine normally after catheter removed • Cardiac consult – small PDA, small PFO, apical VSD • Pelvic ultrasound – no uterus, normal bladder, kidneys • Blood results – • WCC – 14,27 Hb – 16,5 Plts – 159 • U&E – 139 / 3,9 / 104 / 14 / 5,0 / 92 • Hormone levels to be discussed later • To be followed up at endocrine clinic
Ambiguous Genitalia • Manifestation of Intersex Disorders • Characterised by abnormal differentiation, development of external, (sometimes) internal sexual structures • Normal sexual differentiation • Phenotypic sex - genetic/chromosomal sex, follows logical sequence of events • Chromosomal sex established at fertilisation ~ determines gonadal sex • Gonads determine differentiation/regression of internal ducts (Wolffian/Müllerian) • At 6 - 7 weeks gestation: • Y chromosome => undifferentiated gonad=> testis • Absence of Y chromosome => ovary • Processdictated by Testis–determining factor (TDF), product of Sex–determining region on Y chromosome (short arm) • Absence of TDF – ovaries develop • Also autosomal determinants of sexual differentiation • Still unexplained – true hermaphrodites (XX), XX males – no Y chromosome • General rule – Y chromosome necessary for presence of testes
Gonads develop from blastemal mass, primordial germ cells • Leydig cells – testosterone under influence of HCG (placental) and • LH (pituitary) • Week 4 • Wolffian ducts develop, open into cloaca • Müllerian ducts develop later • Both complete by week 8 • Testosterone binds to testosterone–binding androgen receptors, development of epididymis, vas deferens, seminal vesicles • External genitalia respond to Dihydrotestosterone – requires conversion of testosterone by 5 alpha reductase • Anti-Müllerian Hormone (Sertoli cells) – local (paracrine) effects ; • Role in descent of testis • “halts” spermatogenesis at meiosis, continued later at puberty • Regression of Müllerian ducts (9 –11 weeks) • Without AMH, Wolffian ducts disappear, fallopian tubes, uterus, upper 1/3 vagina develop • This occurs with/without ovaries; not affected by androgens
External Genitalia – from genital tubercle, urogenital groove, paired urethral folds, labioscrotal swellings, urogenital sinus (see picture) • Male: • development dependent on 5 alpha dihydrotestosterone • AMH – testes into inguinal region, • testosterone – Wolffian duct derivatives, testes, into scrotum • Female: • Urogenital sinus forms lower 2/3 of vagina • Role of Pituitary and Placenta • Major stimulus to Leydig cells initially placental HCG • After critical period of sexual differentiation, pituitary gonadotrophins responsible for growth of penis • Fetal LH, placental HCG necessary for normal growth of penis, scrotum, descent of testes • Hypopituitarism (congenital gonadotrophin deficiency) – micropenis, bilateral cryptorchidism • Females – placenta major source of oestrogen
Abnormal Sexual Development • Intersex disorders divided into 3 groups: • Virilised females • Undervirilised males • Disorders of gonadal differentiation • 1) Virilised Females • 46 XX, normal ovaries, internal genitalia • Varying degrees virilisation – depends on time, amount of androgen exposure • Early – retention of urogenital sinus, labioscrotal fusion • Later – clitoral hypertrophy • Müllerian duct differentiationnormal • CAUSES: • Fetal androgens - Congenital Adrenal Hyperplasia (CAH) • Maternal androgens – anabolic steroids, Danazol, ovarian / adrenal tumours • Syndromes – Zellweger, Beckwith-Wiedemann • Idiopathic
Congenital Adrenal Hyperplasia (CAH) • Constitutes 60% of all intersex cases in literature (however in South Africa true hermaphroditism is dominant) • Possible medical emergency • Results from block in steroid synthesis pathway – excess of precursors, deficiency of end-product • Decreased negative feedback – increased ACTH – adrenal hyperplasia, pigmentation • Manifestations depend on level of block • (see diagram) • 90% of cases – 21 Hydroxylase deficiency • Salt-wasting, hyperkalaemia, hypotension, vascular collapse • Autosomal recessive
2) Under-virilised males • 46 XY, testes • Causes: • LH Deficiency • Leydig cell hypoplasia • Disorders of testosterone synthesis (testes alone/testes and adrenals) • Abnormalities of peripheral testosterone effects (resistance) • Certain syndromes • 5 alpha reductase deficiency • Converts testosterone to dihydotestosterone (DHT) • Ambiguous genitalia (pseudovaginal perineoscrotal hypospadias), testes present (descended), internal Wolffian duct development normal • Extreme virilisation at puberty, testosterone responsible for male pubertal development • No prostatic enlargement/ acne/facial hair (these depend on DHT) • Diagnosis – high testosterone:DHT ratio (HCG stimulation test – not necessary in newborn)
End-organ resistance (testicular feminisation) • Quantitative/qualitative receptor defects • X-linked recessive inheritance • Complete/incomplete • Complete – female genitalia, no Müllerian structures, short vagina, breasts, no pubic/axillary hair • Many degrees – normal female to various degrees of virilisation • NB – increased incidence gonadal malignancy • Disorders of Gonadal Differentiation • Ovarian and testicular tissue present • 1) Pure gonadal dysgenesis • “streak” gonads – ovarian stroma, no oocytes • Usually XO or XY or XO mosaics • Turner syndrome is an example • 2) Mixed gonadal dysgenesis • Testis on one side (inguinal area or scrotum), streak gonad on other side + Müllerian structures on that side • Most XO/XY • Klinefelter Syndrome
3) True Hermaphrodite • Well-developed testicular and ovarian tissue, same/opposite gonad • Bilateral ovotestes (20%), 1 testis + 1 ovary (30%), or ovotestis + testis or ovary • Wolffian, Müllerian duct development follows lead of ipsilateral gonad • Ambiguous genitalia • Hernia containing gonad/Müllerian duct derivative • 46XX commonest karyotype; mosaicism common • ?Translocation of portion of Y chromosome onto X chromosome or autosome to explain testicular development in absence of Y chromosome
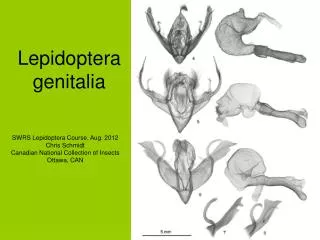
Investigations • Diagnosis important – counsel parents, plan management, treat medical emergencies • History • Genital ambiguity, infertility, unexplained changes at puberty/late onset puberty, previous unexplained neonatal death • Maternal drugs • Maternal virilisation (?tumour) • Examination • Dysmorphic features • External genitalia: • Size, degree of differentiation of phallus (clitoromegaly or hypospadias) • Position of urethral meatus • Fused/separate labioscrotal folds • Scrotal/labioscrotal folds rugose or hyperpigmented
Gonads • ?palpable • Usually only testicular material descends fully • Rectal examination • Cervix, uterus – may be easier in neonatal period • Laboratory Studies • Chromosomal analysis • Endocrine screening – testosterone, DHT, 17 hydroxy- progesterone, dehydroepiandrosterone (DHEA), LH, FSH, ACTH, plasma renin activity, aldosterone (later) • Urea & electrolytes, serum glucose • Androgen receptor levels (genital skin – fibroblast culture) • 5 alpha reductase, type 2 levels • Stimulation tests • Stimulate potential testicular tissue with HCG – highlights altered testosterone:DHT ratio • ACTH stimulation
Imaging • Pelvic ultrasound • Difficult, need full bladder • Uterus, Mullerian structures, adrenal gland enlargement (cribriform appearance) • Uterus present – usually virilised female • Absent uterus – more difficult • Genitogram • Ductal anatomy • Contrast injected into urogenital sinus • Other • CT scan, MRI, exploratory laparotomy/ laparoscopy, gonadal biopsy
Management • Medical – • Supportive in CAH, replacement of hormones • Surgery – • Timing, type controversial • Issue of gender assignment often very difficult, emotional, requires team approach • Virilised females – feminising genitoplasty • Undervirilised males – correction of hypospadias, gender reassignment • Dysgenetic/non-functional gonads – require removal, high risk malignant change by 4th decade • Karyotype not necessarily determinant in gender reassignment
What have we learned in this case? • Chromosomes 46XY • Results (13/08/2003) • Testosterone – 3,8nmol/l (normal) • LH - <0,1IU/l (normal) • 17OH Progesterone – 1,3nmol/l (normal) • Cortisol – 319 (normal) • DHEA(S) – 0,9umol/l (low) • Post HCG Stimulation Test • Testosterone – 6,4 nmol/l • Assessment • Undervirilised male, normal testicular tissue • ? 5 alpha reductase deficiency