Download
1 / 49
1.74k likes | 8.59k Views
Ambiguous Genitalia. By Dr Raed Azhar MD & Dr Ashraf Abusamra MD, FRCSC, FSUO. Outline. Introduction. Mechanisms of Sexual Differentiation. Differential diagnosis of a newborn with ambiguous genitalia. Congenital Adrenal Hyperplasia (CAH). Approach to a baby with Ambiguous Genitalia.

E N D
Ambiguous Genitalia By Dr Raed Azhar MD & Dr Ashraf Abusamra MD, FRCSC, FSUO
Outline • Introduction. • Mechanisms of Sexual Differentiation. • Differential diagnosis of a newborn with ambiguous genitalia. • Congenital Adrenal Hyperplasia (CAH). • Approach to a baby with Ambiguous Genitalia.
Introduction • Disorders of Sexual Differentiation: - Newborn period with Ambiguous genitalia. - Inappropriate pubertal development. - Delayed pubertal development. - Later in life with infertility. • The evaluation of the newborn with ambiguous genitalia is a medical & social emergency.
Mechanisms of Sexual Differentiation • Series of staged modifications of B/L tissue primordia. • These modifications appear to be controlled by local factors, independent from one side to the other. • Development of gonads. • Development of internal ducts. • Development of external genitalia.
Development of Gonads • The genetic sex is determined at the time of fetilization by the delivery of an X or Y chromosome by the sperm. • The medullary portion of the indifferent gonad develops into a testis under the influence of testis-determining factor (TDF) that present in the short arm of Y chromosome. • In the absence of TDF, the cortex of the indifferent gonad develops into an ovary. • By the 7th week of gestation the gonadal sex is established.
Development of Internal Organs • By 6th wk of GA, 2 paired internal duct systems derived from the mesonephric renal system exist side by side. • The mesonephric (wolffian) duct M structures. • The paramesonephric(mullerian)duct Fstructures. • M differentiation is dependent on testicular production of MIS from fetal sertoli cells & testosterone secretion by fetal Leydig’s cells.
Development of Internal Organs (cont.) • Following regression of the mullerian duct under the influence of MIS, the wolffian duct will develop into epididymis, vas defrence, & seminal vesicles under effect of testo. • In the absence of MIS & testo. The mullerian duct will evolve into fallopian tubes. uterus,& upper third of vagina.
Development of External Genitalia • Develop from the urogenital sinus, genital tubercle, genital folds, & genital swellings. • Male development is dependent on the ability of these tissues to convert testo, to DHT by the enzyme 5α reductase. • Female differentiation is essentially the unmodified embryologic state that persists in the absence of these hormones.
Classification of Ambiguous Genitalia • Female pseudohermaphrodite. • Male pseudohermaphrodite. • True Hermaphroditism • Gonadal Dysgenesis.
Female pseudohermaphrodite • Virilization of 46XX genetic female with N ovaries 2ry to excessive endogenous or exogenous intrauterine androgens. • Commonest cause of ambiguous genitalia. • 95% due to CAH. • 5% due to exposure to maternal androgens(e.g maternal ingestion of certine progestins,or maternal virilizing tumors such as arrhenoblastomas or luteomas).
Male pseudohermaphrodite • Incomplete virilized 46XY with N testes. • Causes: defective androgen synthesis or action, def. 5 α reductase activity, or def. MIS ( Herni uteri inguinale). • If the androgen defect is severe, pts may have complete feminine external genitalia with intra abd testes (complete test. feminization).
Male pseudohermaphrodite: Hernia uterine inguinale,or persistant mullerian duct syndrome. Note the presence of fallopian tube & uterus attached to the testicular cord structures.
True Hermaphroditism • Rare. • Both testicular & ovarian tissue are present. • Commonest karyotype 46XX (80%). • The Internal genitalia correspond to the sex of the ipsilateral gonad. • External genitalia commonly masculinized with large phallus with chordee & hypospadius is common.
True hermaphrodie : On the pt’s Rt side,note the testes, & on the Lt. note the fallopian tube, uterus, & Bx proven ovary.
Gonadal Dysgenesis • The 2nd commonest cause of ambiguous genitalia • Disordered development of the gonads. • The gonads often are replaced by fibrous streak. • Commonest karyotype : 46XY/45XO mosaic. • 25% will develop testicular gonadoblastoma.
Gonadal Dysgenesis (cont.) • Spectrum of presentations: - Pure gonadal dysgenesis (e.g Turner’s syndrome both ovaries are replaced by fibrous streak). - Mixedgonadal dysgenesis : the commonest cause, 1 gonade a fibrous streak & the other is testicle. - Testicular dysgenesis (testes are purely dysplastic)
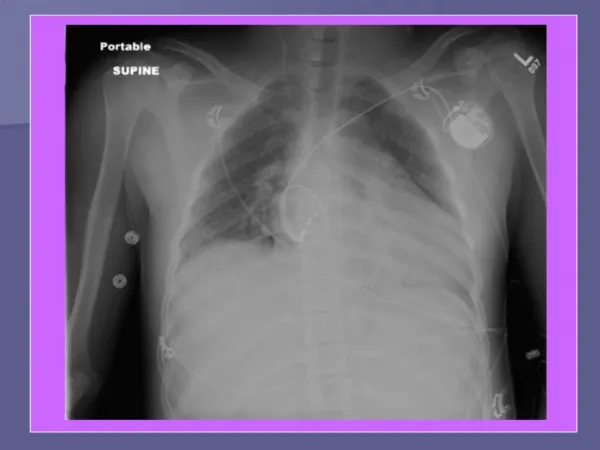
Mixed gonadal dysgenesis: with ambiguous genitalia & a unilateral palpable gonad on the Rt. Side.
Differential diagnosis of a newborn with ambiguous genitalia
Congenital Adrenal Hyperplasia (CAH)
CAH • Commonest cause of female ambigious genitalia. • 70% of all pts with ambigious genitalia. • Autosmoal recessive disorders resulting from def. in one of 5 enzymes (CYP) of cortisol biosynthesis. • CYP : cytochrome P-450 enzyme located in the endoplasmic reticulum & involved in cortisol biosynthesis.
CAH - Biochemistry • >90% due to 21-hydroxylase deficiency (CYP21) inability to synthesize cortisol ↑stimulation of adrenal gland by the pituitary & hypothalamus ACTH ↑ androstenedione. • Androstenedione is metabolized to testosterone & DHT, resulting in virilization of females. • Other causes of CAH; 11b-hydroxylase (5-8%) and 3b-hydroxysteroid dehydrogenase deficiency (<5%) are rare.
Clinical Manifestations • Classic form : salt wasters (virilization & aldosterone def.) • Simple virilizers (virilization, no salt wasting). • Nonclassic (present after puberty with virilization).
CAH -The Classic Form • ↓ levels of cortisol & aldosterone ↓Na, ↑K, acidosis,↑ plasma renin, dehydration, CVS collapse if untreated.
CAH-The Classic Form (cont.) • Severe degree of virilization with Clitoromegaly. • Labial fusion with single perineal opening for vagina & urethra representing a urogenital sinus • Mullerian structures preserved due to lack of AMH. • External genitalia of affected males are generally N. • Progression of masculinization of untreated female.
CAH - Simple Virilizing Form • ↓ cortisol but N aldosterone Na balance N. • In females : ambiguous genitalia at birth. • In males : If not screened, Dx is delayed for several years with signs of androgen excess.
CAH - Non Classic Form • N cortisol & aldosterone, mod ↑ sex hormones. • Few pts are detected by screening. • Some children grow rapidly, some have pubic or axillary hair prematurely. • Adult female: Hirsutism 60%,oligomenorrhea 54%,acne 33%, infertility 13%.
Diagnosis of CAH • 75% of infants have salt wasting ( Na+: ↑ K+) due to lack of mineralocorticoid • Weight loss, dehydration & adrenal crisis • Elevated 17oh-progesterone 48 hrs after birth • Many countries screen newborns for CAH (filter-paper blood spot test for 17oh-progesterone) • Prenatal tests for at-risk pregnancies include e.g amniocentesis : • Karyotype • mutation analysis of 21-hydroxylase gene CYP21. • Amniotic fluid 17oh-progesterone measurement
CAH – Antenatal Treatment • Should begin at 6 wks of gestation; it is not possible to confirm diagnosis before ttt. • Prenatal administration of dexamethasone >> suppress fetal ACTH >> prevent virilization of suspect female fetuses. • Only mothers carrying affected females need to continue treatment • Both alleles must carry CYP21 mutation • Males do not require antenatal treatment • 7/8 fetuses are initially treated unnecessarily • Blocks virilization in most females • Side-effects are minimal
CAH – Medical Management • Glucocorticoid replacement with hydrocortisone. • Mineralocorticoid replacement with fludrocortisone. • Plus salt supplements. • Problems in later life: obesity, menstrual irregularities, reduced stature & infertility
CAH – Surgical Management • Feminizing clitoroplasty &/or vaginoplasty • In females, feminization, menstruation & fertility can be anticipated in well-treated patients • Long-term fertility in males • For 25% of CAH patients who completely lack 21-hydroxylase activity (produce neither cortisol nor aldosterone), adrenalectomy may be indicated.
Approach to a baby with Ambiguous Genitalia • Adequate History - Family history: neonatal death, infertility, amenorrhea - Exposure to teratogenic compounds - Maternal steroid ingestion • Physical Examination 1- Document degree of external virilization ** • Prader 0 – Normal female anatomy • Prader 1 – Enlarged phallus • Prader 2 – Separate urethral & vaginal openings • Prader 3 – single urogenital sinus opening • Prader 4 – enlarged phallus with hypospadias • Prader 5 – Normal male anatomy **Predicts extent of early androgen exposure
Approach to baby with Ambiguous Genitalia # Physical Examination 2 - Examine urogenital sinus for presence of vagina • early androgen >> vaginal regression • Determine presence & location of gonads • Palpable gonads predict testicular development & ipsilateral Mullerian regression • Palpable gonads are testes baby is undervirilized male • Differential Diagnosis: - Inadequate testosterone - Receptor deficiency - 5a-reductase deficiency - Gonadal dysgenesis -True hermaphrodite
Approach to a baby with Ambiguous Genitalia • One gonad palpable; other may be ovary, ovotestis or streak; hemi-uterus likely present • Consider: - True hermaphroditism - Mixed gonadal dysgenesis Bilateral impalpable testis or unilateral impalpable testis with hypospadias >>> Intersex disorder MUST be ruled out
Intersex – Investigations • Radiological Imaging - Pelvic US to detect presence of uterus/cervix may detect gonads. - Urogenital sinogram to define lower vagina. - MRI may be used to locate gonads. • Chromosome karyotype from peripheral leukocytes to determine genotype or mosaicism • U&E to exclude salt wasting CAH. • 17oh-progesterone after 48 hrs is elevated in CAH • Serum testosterone & DHT (ratio reflects 5a-reductase activity)
Intersex – Investigations • Other Hormonal Tests - Serum gonadotropins. - hCG stimulation test as a marker of functioning testes & whether they produce androgens. - Estradiol levels after stimulation with human menopausal gonadotropin confirms the presence of ovarian tissue. - Serum AMH is a reliable marker of the presence of testes, since it is a product of Sertoli cells.
Intersex – Investigations • Gonadal biopsy is only required when a firm diagnosis based on the aforementioned data is impossible
The diagnostic significance of gonadal position & presence of uterus in babies with ambiguous genitalia
The diagnostic significance of gonadal position & presence of uterus in babies with ambiguous genitalia
References • Campbell’s Urology – 8th edition. • Smith’s General Urology – 16th edition. • Urology Pearls by Sahn & Heffner. • The 5-minute Urology consult. • Congenital Adrenal Hyperplasia, review article by Phyllis W. speiser, The New england Journal of Medicine 2003; 349:776-88. • www.emedicine.com