Download
1 / 35
350 likes | 906 Views
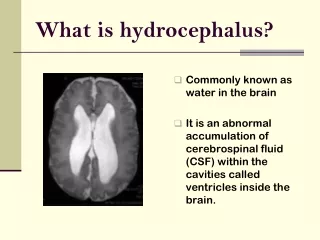
Hydrocephalus. Hydrocephalus is a condition where there is an imbalance between the production of cerebrospinal fluid and its absorption over the surface of the brain and into the circulatory system . Cerebrospinal fluid is constantly produced to protect the brain and spinal cord.

E N D
Hydrocephalus is a condition where there is an imbalance between the production of cerebrospinal fluid and its absorption over the surface of the brain and into the circulatory system. • Cerebrospinal fluid is constantly produced to protect the brain and spinal cord. • If there is a blockage, the fluid accumulates and causes swelling and pressure against the brain tissue hydrocephalus will be the consequence of this. • As the amount of fluid in the brain increases the head size increases within babies and young children whose bones are still flexible and not yet fused.
Causes • Congenital Occurring at birth but the reasons are often unknown • Prematurity A premature baby is very vulnerable. The brain is still developing; blood vessels are fragile and easily damaged. If a blood vessel bursts, a clot may occur, causing a blockage of the cerebrospinal fluid. • Spina bifida Babies born with spina bifida may also develop hydrocephalus. In addition to the lesion in the spinal cord, there may be other abnormalities in the structure of the brain, which prevent adequate draining of the cerebrospinal fluid. • Meningitis: Meningitis is the infection of the meninges or linings of the brain and spinal cord. This results in swelling of the meninges, thus blocking the draining of the cerebrospinal fluid. • Brain and spinal tumours: Brain and spinal tumours cause compression and affect the drainage of the cerebrospinal fluid.
Characteristics • The characteristics of this condition will vary depending on the individual. • As stated above the child with increased fluid will have flexibility in the skull as the bones have not yet fused which will allow for some increased amounts of CS fluid. • Babies with hydrocephalus may have a rapid growth in head circumference – which is why the public health nurse will be checking the size of the baby’s head when doing their visits in the early months of life. • Difficulties may also include vomiting and seizures.
As the bones of the skull fuse and close different difficulties will occur; such as • blurred or double vision, • poor coordination, • difficulty with balance and walking, • urinary incontinence • slowing of developmental progress. • Visual Impairments: Squint, nystagmus (rapid, involuntary eye movement) • Hearing Impairments: A child may be very sensitive to noise • Touch and Taste: A child may experience difficulties with shape, texture, temperature and taste.
Learning Difficulties: The child may present with specific learning difficulties • Short attention span • Poor short-term memory • Spatial awareness and visual perception difficulties • Sequencing difficulties • Delayed fine motor control • Behavioural Difficulties • It is important to remember that each child will present with a different level of difficulties.
Treatment • On diagnosis of hydrocephalus, the child will receive surgical treatment to insert a shunt. • The shunt system is a flexible plastic tube which consists of the shunt, the catheter and the valve. • A shunt system acts as a valve and directs the flow of cerebrospinal fluid from the obstruction or blockage into the bloodstream. • The upper part is inserted into the brain and the lower part into the heart or abdomen. • The fluid flows through the tubes and into the bloodstream.
The shunt system is not obvious to the onlooker, as it is completely enclosed in the child’s body. • The shunt does not cure hydrocephalus, but helps to prevent any further brain damage. • The shunt will require monitoring to ensure it is functioning correctly. When complications occur the failed element of the shunt will be replaced. • The failure of the shunt may occur due to over draining where the shunt allows the fluid to drain more quickly than it is produced which can cause the ventricles to collapse causing headaches, vomiting or haemorrhaging. • The failure may also occur if the shunt drains the fluid too slowly causing the build-up the cerebrospinal fluid thus causing the reoccurrence of hydrocephalus symptoms.
When working with the child with hydrocephalus: • A major role of the SNA is to watch out for signs that may indicate something is wrong with the shunt. This will usually be a blockage or an infection. Surgery is necessary for the treatment of both blockage and infection. • :
Indicators may include • Headache • Vomiting • Fever • Irritability / sleepiness • Personality change • Loss of bladder and bowel control • Staggering • Seizures • Lethargy Observation of any of these should be reported to the teacher immediately.
When working with a child with hydrocephalus it is important to meet his learning and emotional needs in addition to his physical needs. • Ensure that the child is comfortable and that any equipment for activities is accessible. • Encourage activities that stimulate the senses • Physical activities help to release tension and develop spatial awareness.
What is the role of the Special Needs Assistant when working with a student with a Physical Disability
Until quite recently children with physical disabilities would have attended special schools as the facilities were not available for this child in the mainstream school. • Thankfully also with this change in accessibility, concepts and ideas of disability have changed greatly and are much more positive today. • All children are individuals with specific needs and wants, children with physical disabilities will differ in the severity of their condition and therefore their needs. • As special needs assistants working with children with physical disabilities we must have knowledge and understanding of the following:
Have a good knowledge of the disability and its severity (specifically related to the child with whom you are working) • You will need information about associated learning difficulties if they are present • Make sure you are aware of all the implications of the disability (behavioural, emotional etc) • Students with cerebral palsy will have different degrees of mobility. Some may use a walking frame while others will be wheelchair users. Some of these students will need help writing and turning pages of a book while some may have difficulty eating or speaking
Have sufficient knowledge of what triggers certain conditions such as students with cerebral palsy who also have epilepsy. • You should know what type of epilepsy the child has (e.g. photosensitive epilepsy- here when the teacher is showing a DVD for example you would need to know if strobe lighting was used in the film before the child would watch it as this would be a trigger)
Help the child with their mobility if needed and have a good knowledge of the correct use of equipment • You will need to promote their independence skills (aiding them to complete tasks themselves rather than completing tasks for them which will make them more dependent on you)
Help the child to master skills such as feeding where possible with correct training • Have a working knowledge of the equipment that the student is using • Ensure you know the correct lifting techniques • Ensure you see the child’s abilities first and not focus on their disabilities. • Do not talk over the child and do not do all the talking for the child
You need to have knowledge of the following: • Pupils with cerebral palsy may have difficulty perceiving visual images • The student with hydrocephalus sometimes has mood swings and tires very easily • Pupils with spina bifida sometimes have poor fine motor control
Administering Medication • Please remember that only the designated person on the safety/medical policy can administer medicines. • Read instructions to know exact dosage, the role of administration and correct time to administer medicine • If pouring – pour in good light to ensure you are giving the correct amount • If medication
Never pour any excess liquid back into the bottle as contamination may occur • Make sure the child has taken medication and not held it in their mouth • Keep a record of when medicine was administered –with details of amount and to whom • When giving medicine to a person with cerebral palsy remember then may have difficulty swallowing depending on the areas affected by this condition. In this case you must ensure they have plenty of fluid to assist in the swallowing process
Wheelchair users • Do: Listen to the child remembering to ensure they are not in any discomfort Talk to the child while aiding their movement • Check the child’s clothing is tucked away from the wheels to prevent an accident Ensure that you are speaking clearly and at a level the child can understand • Don’t: Rush when pushing the wheelchair. Always push at an even pace Forget that the child is in the wheelchair and include them in whatever is happening
MOTOR DYSPRAXIA (DCD) • Developmental Co-ordination Disorder (DCD) is the term used internationally to describe coordination difficulties in children. • Dyspraxia refers to a specific disorder in the area of motor skill development where children with dyspraxia have difficulty planning, sequencing and completing co-ordinated movements appropriate to the norms expected for the child. • Currently there are no official statistics of prevalence of DCD in Ireland, however, the Dyspraxia Association of Ireland in 2005 suggested 6% prevalence rates for children in Ireland. More boys present with this condition than girls in the ratio of approximately 4:1.
Causes • While the cause of DCD is still unclear to a great extent it is known to be a neurological disorder and is caused in part by poor processing of information in the brain. Other research suggests that it may be caused by • Lack of oxygen around the time of birth (much research is still underway focusing on this theory) • Early viral infection • Some research has focused on the fact that premature births may lead to a failure of the neurons in the brain forming correct connections • There has also been focus placed on a hereditary link • It is important to note that research is still on-going in this area
Diagnosis • D.C.D. is only diagnosed when a child has unexpected difficulties doing activities involving coordination and movement. • Diagnosis involves assessing the child over a range of skills which require co-ordination skills such as riding a bike, buttoning a shirt, writing etc. • For the diagnosis to take place the child must have significant difficulties in motor co-ordination which affects both home and school life. • Sometimes this condition may accompany specific disabilities such as cerebral palsy or a learning disability.
Characteristics • There are many characteristics which are prevalent at differing stages of development. Below are a sample of these difficulties. • Characteristics can be seen from an early stage with babies often having significant feeding problems. As stated above they are slow to achieve developmental norms expected. • Many children with dyspraxia fail to go through the crawling stages, like those with specific learning disabilities missing this stage of development which is crucial for co-ordination.
As the child reaches school age the following characteristics may be noted. • (It is imperative as with all difficulties to get diagnosis at an early stage so that interventions can begin) • Poor balance/posture • Inability to sit still (fidgeting constantly) • Concentration difficulties (poor attention span) • Difficulties in adapting to a structured school routine • Difficulties in physical education lessons (ball games)
Difficulty riding a bike due to balance and co-ordination difficulties • Poor fine motor skills. Difficulty in holding a pencil or using scissors. Drawings may appear immature. Handwriting may be difficult to read. • Confused about which hand to use. • Intolerance of having hair or teeth brushed, nails and hair cut. • Organisational difficulties in tasks • Slow at dressing. Unable to tie shoe laces
Inability to remember more than two or three instructions at once • Slow completion of class work • Difficulty with social skills and often relating to peers • Listening skills are a difficulty • Sleeping difficulties
Associated Conditions • This will vary depending on the child. • Learning difficulties such as dyslexia • Behavioural problems • Speech and language difficulties
Treatment • This difficulty was often called “clumsy child syndrome” in the past and it was believed that children “grew out” of this stage. • However, current studies being undertaken suggest that this condition may prevail to some degree throughout the life span of the person with this condition.
Occupational Therapist • This therapist will help with the daily living skills of the child with dyspraxia. This therapist will look at working on movement, balance, posture and organisation skills. They may use Sensory Integration Therapy.
Sensory Integration Therapy • This treatment involves working on the child’s reflexes, postural control, balance, bilateral coordination, tone and general movement abilities. • By working on the underlying areas of weakness, the child’s skills at more complex levels improve, e.g. if a child has difficulties in staying seated, it can be due to poor postural control. • Through sensory integration he can be helped to strengthen his tone and muscle control and so develop better stamina for sitting at his desk.
Therapeutic Listening • This therapy is specialised and treatment differs depending on the specifics of the child’s difficulties. • It is a form of auditory intervention. • The therapy involves using music and the Electronic Ear (Dr. Alfred Tomati) As stated, this individualised programme is dependent on the needs of each child. For more information on this form of therapy please go to the Cluas website http://www.cluas.ie
When working with the child with Motor Dyspraxia (DCD): • The following areas can be worked on effectively by the special needs assistant in conjunction with the teacher; • Help the child practise skills such as: tying shoe laces, opening their lunch box, hanging up their coat, forming letters, cutting using a scissors • Help them practise skills such as throwing a ball, catching a ball, jumping and hopping • Keep distractions to a minimum • Ensure that all instructions given are understood (do not overload the child)
Encourage the child to keep belongings in a particular place all the time, to aid with organisation. • Ensure the child has all homework written down and that all books required for this work go home with them