Download
1 / 27
270 likes | 308 Views
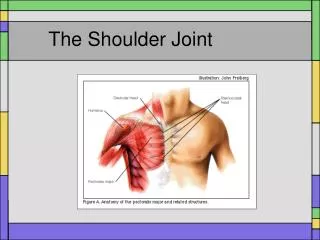
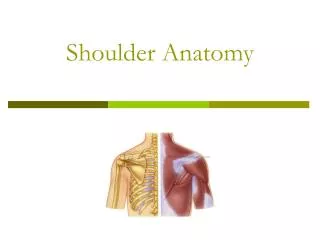
Shoulder Joint-Anatomy (1). Sternum Clavicle Scapula- acromion process and coracoid process, glenoid fossa and glenoid labrium, spine of scapula Humerus- Greater tubercle, Lesser tubercle, head of humerus, http://www.readingshoulderunit.com/shoulder_anatomy.htm. Shoulder Anatomy (2).

E N D
Shoulder Joint-Anatomy (1) • Sternum • Clavicle • Scapula- acromion process and coracoid process, glenoid fossa and glenoid labrium, spine of scapula • Humerus- Greater tubercle, Lesser tubercle, head of humerus, • http://www.readingshoulderunit.com/shoulder_anatomy.htm
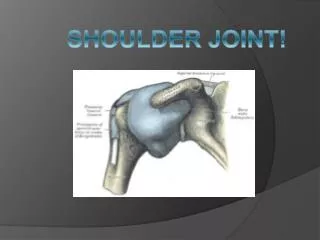
Shoulder Anatomy (2) • The shoulder encompasses 5 separate articulations • Sternoclavicular (SC) joint • Acromioclavicular (AC) joint • Coracoclavicular joint • Glenohumeral (GH) joint • Scapulothoracic (ST) joint
Sternoclavicular (SC) Joint ** • Joint between the sternum and clavicle • Allows for rotation during movements like shrugging the shoulders and reaching above the head. • Supported by 4 ligaments- Fig 8-1 • anterior and posterior SC ligament • Costoclavicular ligament • Interclavicular ligament
Acromioclavicular (AC) Joint** • Lies between the acromion process and the clavicle • Has limited motion • Primary ligament: AC ligament • Secondary ligaments • Coracoacromial ligament • Coracoclavicular ligaments
Glenohumeral (GH) Joint**(1) • Fig 8-2 • “true” shoulder joint • Glenoid fossa of the scapula • VERY shallow • Head of the humerus (3-4 x larger than glenoid)-plunger/volleyball example • lacking in bony stability
GH joint** (2) • Joint is deepened by a meniscus like structure called the glenoid labrum • functions to add stability to the joint • Stabilized by two types of stabilizers • Static stabilizers • joint capsule • several glenohumeral ligaments
GH joint** (3) • Dynamic stabilizers • rotator cuff muscles (SITS) • Supraspinatus • Infraspinatus • Teres minor • Subscapularis
Scapulathoracic Joint** • Gliding joint • Scapula rotates to allow full abduction and adduction • Called Scapulothoracic rhythm • Several important muscles are stabilzers including the: • levator scapula, rhomboids, trapezius, and serratus anterior
Other shoulder anatomy (3) • Bursa • Subacromial (clinically most important) • Nerve supply • brachial plexus (C5-T1) • Blood supply • subclavian, axillary artery
Shoulder movements • Flexion (180) and Extension (80-90) • Abduction (180) and Adduction • Horizontal Adduction/Flexion (130) • Horizontal Abduction/Extension (60) • External rotation (90) • Internal rotation (90)
Throwing Motion Activity • Cocking, Acceleration, Deceleration • Flexion, Extension, Hyperextension • Abduction, Adduction • Horizontal Adduction/Flexion • Horizontal Abduction/Extension • External rotation, Internal rotation • Elbow Extended, Elbow Flexed
Anatomy of throwing • Three phases of over arm throwing- Fig 8-10 and Box 8-1 • Preparatory or cocking phase • Acceleration or delivery phase • Deceleration or follow-through phase • Shoulder goes thru over ???°/sec-knee ???°/sec when walking • Common injuries during the throwing motions Box 8-2
Cocking phase • Arm in horizontal abduction, hyperextension and external rotation • eccentrically loaded: • horizontal adductors • internal rotators • scapular muscles • rhomboids pull scapula back • serratus anterior stabilizes the scapula
Acceleration or delivery phase • Ball brought forward and released • humeral horizontal add, elbow extension, rapid internal rotation • romboids relax • Large stresses placed on ligaments,
Arm deceleration/ follow through • After ball release, until maximum shoulder internal rotation, horizontal adduction are reached • Eccentric loads placed on: • infraspinatus, supraspinatus, teres major and minor, lats, posterior deltoid
Preventing shoulder problems • General muscle strengthening • Try and avoid exercises above 90 degrees • Stretching for shoulder capsule, but be careful • Strengthening rotator cuff muscles • including eccentric work • http://www.asmi.org/SportsMed/throwing/thrower10.html • Throwing Program • Strengthen scapular stabilizers • push-ups • press-ups
SC joint Sprain • MOI: direct blow to clavicle or transition forces from a blow to the shoulder driving the clavicle out of place • HOPS • point tenderness over SC joint • bruising, swelling and pain over SC joint • deformity increases with degree; posterior is serious • Motion decreases with degree • TX-See Field Strategy 8.4
AC joint sprain • “Separated Shoulder” • MOI: fall on tip of shoulder, direct blow to the tip of the shoulder, falling on outstretched hand (FOOSH) HOPS • point tenderness over AC joint • bruising, swelling and pain over AC joint • deformity increases with degree; or step deformity • Piano key test positive in 3 degree • TX: place in sling, x-ray; Field Strategy 8.5
GH joint sprains • Two forms: • Acute Dislocations • Recurrent subluxations/ dislocations • Acute Dislocations • MOI: external rotation, abduction, extension • Most are anterior dislocations • may cause a avulsion of the anterior portion of the glenoid = Bankart lesion
Acute Dislocations (con’t) • HOPS • Intense pain • Tingling and numbness down arm into the hand • arm held at slight abduction, external rotation, and stabilized against the body • Flattened appearance to the shoulder; acromion process becomes prominent (Fig 8-14) • inability to move shoulder • Tx-check neurovascular status, sling and ice if able; referral; DO NOT REDUCE
Chronic dislocations/ subluxation • MOI: same as acute, force required is less • HOPS: • less symptoms than acute • “dead arm syndrome” • TX: • conservative: therapy • surgery if needed
Rotator Cuff impingement (1) • Involves several structures: • supraspinatus tendon micro-tears • subacromial bursa • coracoacromial ligament • Glenoid labrum • long head of bicep • May lead to rotator cuff rupture if unchecked
Rotator Cuff impingement • MOI: repetitive microtrauma (overuse) • HOPS: • pain with activity • pain with overhand motions • painful arch (between 70 and 120 degrees of AB) • Inability to sleep on involved side • + supraspinatus tests, impingement test • TX: TX: cryotherapy, NSAID’s, rest, gradual strengthening, retraining of muscles
Bicipital Tendonitis • MOI- overuse during rapid overhead movements with excessive elbow flexion and supination; • Bicep tendon gets irritated in the bicipital groove and may partially sublux • HOPS-pain in anterior aspect of shoulder over the bicipital groove; athlete may say something is “popping”; pain with resistive elbow flex and supination and passive stretch of bicep • Tx- rest from motions that aggravate, ice, NSAID’s, strengthening and stretching
ROM/Muscle Testing • Shoulder flexion-Ant Delt/Pec Major • Shoulder extension-Post Delt • Shoulder abduction-Middle Delt • Shoulder adduction-Pec Major/Lats • Shoulder internal rotation-Ant Delt/ Subscapularis • Shoulder external rotation-Infraspinatus/ Teres Major • Horizontal ADD/Flex-Ant Delt • Horizontal ABD/Ext- Post Delt • Scapula elevation, depression, protraction, and retraction
Special Tests • Apprehension test (shoulder dislocation) • Empty Can and Drop Arm Tests (supraspinatus) • Impingement (impingement) • Yergerson’s (biceps tendinitis)
HOPS • History • Observation • Palpation