Download
1 / 15
160 likes | 227 Views
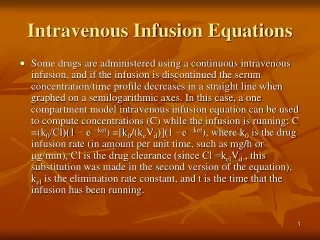
Intravenous Infusion. Intravenous Infusion Policy Overview. Only vessels in the upper extremities are approved venipuncture sites . Other sites may only be used with a written physician order.

E N D
Intravenous InfusionPolicy Overview • Only vessels in the upper extremities are approved venipuncture sites. • Other sites may only be used with a written physician order. • Once the IV or TPN has been infused the nurse will peel off the HIPAA strip which will render the patient’s name illegible and discard the bag
IV Rates • All IV admixtures ordered to be infused as KVO will have a rate of 10ml/hour • All KVO IV solutions shall be changed at least every 24 hours • KVO solutions without additives may be automatically substituted with a saline lock • Dextrose 10% may be hung on patients 6 years of age or older in lieu of an ordered TPN solution until the solution is prepared. The dextrose solution can hang only a maximum of 8 hours.
Infection Control • Tegaderm dressing over the IV site must be changed every 96 hours • No antibiotic ointment • If a gauze dressing is used it should inspected every 8 hours and changed every 24 hours
IV Site Changes • Peripheral venous-every 96 hours • CVP lines, peripheral arterial, pulmonary arterial (peripherally inserted, hemodialysis & umbilical should not be replaced routinely) IF for any reason a nurse is unable to restart the IV, the nurse should seek assistance from another nurse. If still unsuccessful, the nurse should notify the rapid responder nurse and then the appropriate house officer for orders.
IV tubing and extension tubing is changed & labeled every 96 hours IV tubing for lipids & hyper alimentation is changed & labeled every 24 hours Tubing for A-line and Swan lines are changed & labeled every 96 hours
Documentation • EMR • IV flowsheet • Intake and Output • MAK • CMR - Downtime
IV Push Medication AdministrationPolicy Overview • RN’s on general medical-surgical patient care units may give approved IV push drugs listed on the IV Push Medication Guidelines Sheet from pharmacy (refer to the actual policy) • RN’s on specialty areas may have additional or differing medications & doses (refer to specific policy, procedure or protocol)
IV push medications not on the approved “IV Push Medication Guidelines” sheet must be administered by the physician. Prepare the medication - leave the medication container and MAR out for the physician to check. After the physician administers the nurse will document in MAK the name of the physician that administered the medication The Critical Care RN may be contacted to push IV medication in lieu of House Officer
IV Push Guidelines • Antineoplastic agents are administered only by RNs educated to do so. • Emergency IV Push Medications may be administered by a licensed nurse in the presence of a physician. • Medications are not given directly into the vein - always into an established patent IV line.
IV Push Guidelines IV sedatives & analgesics should not be administered if: • BP has decreases 30mm Hg systolic from the previous reading • BP is 70mm Hg or below • Respirations have decreased to 10 breaths/minute or less
Heparin ProtocolCardiac & Weight Based • Physicians ordered is required to specify: • Weight –Based or Cardiac- Based • Heparin must be the primary IV • Obtain the first PTT per order, usually 6 hours after initiation of Heparin • Adjust Heparin drip based on the PTT results as directed by the nomogram
Revise Heparin Order • Select TO/VO orders: • Click / highlight last active Heparin order • Select “revise” tab on the left • Select attending physician or the physician managing heparin gtt and select “protocol order” then click “ok” • Click “enter order changes” at the bottom right of screen • DO NOT CHANGE WEIGHT IF USING CARDIAC BASED PROTOCOL. If using weight based protocol, enter CURRENT weight. • Select “Titrate” • Enter new rate based on Nomogram • Under Titration Instructions type PTT result, changes to be made, time of next ptt. • Keep duration at 30 days • Click “ok” • Place next PTT as separate, timed order