Download
1 / 17
170 likes | 449 Views
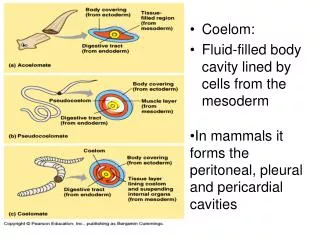
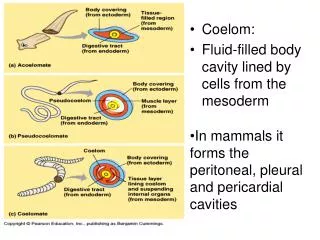
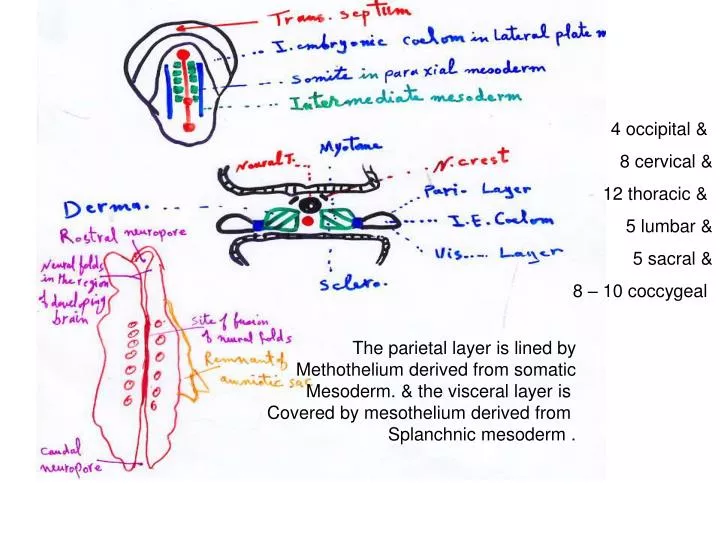
4 occipital & 8 cervical & 12 thoracic & 5 lumbar & 5 sacral & 8 – 10 coccygeal. The parietal layer is lined by Methothelium derived from somatic Mesoderm. & the visceral layer is Covered by mesothelium derived from Splanchnic mesoderm.

E N D
4 occipital & 8 cervical & 12 thoracic & 5 lumbar & 5 sacral & 8 – 10 coccygeal The parietal layer is lined by Methothelium derived from somatic Mesoderm. & the visceral layer is Covered by mesothelium derived from Splanchnic mesoderm .
Early in the 4th week, the intraembryonic coelom appears as a horseshoe-shaped cavity. The curve at the cranial end of the embryo represents the future pericardial cavity & limbs indicate future pleural ;peritoneal cavities . The distal part of each limb of intraembryonic coelom is continuous with extraembryonic coelom at lateral edges of embryonic disc .This communication is important to midgut development. At 6th W herniation occure withen the umblical cord. And at 10th week this connection is lost . The intraembryonic coelom becomes the embryonic body cavity during 4th week ( 22-28 days ) 1. Pericardial cavity 2. two pericardioperitoneal canals 3. peritoneal cavity .
During formation of the head fold , the heart& pericardial cavity move ventrocaudally, anter. to the foregut As a result , the pericardialcavity opens into pericardioperitoneal canals, which pass dorsal to the foregut & on each side of it ( future esophagus ) and dorsal to septumtransversum ( a thick plate of mesodermal tissue ) that occupies the space between thoracic cavity & yolk stalk ) Partitions is formed in each pericardioperitoneal canal that separate pericardial cavity from pleural cavities & pleural cavities from peritoneal cavity. These partition are pair of membranous ridges that is produced in the lateral wall of each canal. The cranial ridges: pleuropericardial folds, located superior to lungs. Caudal ridges: pleuroperitoneal folds are located inferior to developing lungs .
An extention of the visceral peritoneum covering an organ form the mesentery. So , themesentery is a double layer of the peritonium . It connect the organ to the body wall & conveys vessels & nerves to it . The ventral and dorsal mesenteries divide the cavity into R & L halves The venteral mesentere. Disappears , except where it is attached to the caudal part of the foregut ( primordium of terminal part of esophagus , stomach & 1st part of duodenum) . After this level the peritoneum cavity becomes continuous space
The venteral mesentery degenerates , resulting in a large embryonic peritoneal cavity extending from the heart to the pelvic region .
Pleuropericardial Mermbranes They project into the cranial ends of the pericardioperitoneal canal The bronchial buds grow laterally from the caudal end of the trachea into pericardioperitoneal canals ( future pleural canals). As the primordial pleural cavities expand ventrally around the heart, they extend into the body wall , spilitting the mesenchyme into :Anouter layer that becomes the thoracic wall .& Aninner layer (pleuropericardial membrane), that becomes the fibrous pericardium . ( the outer layer of the pericardial sac enclosing the heart ) They contain the common cardinal veins & phrenic Ns. They become mesentery like folds ( extending from the lateral wall of thoracic wall ). This is due to 1. Growth of common cardinal v., descend of heart ; expansion of pleural cavities
By the 7th week , the pleuropericardial membranes fuse with mesenchyme ventral to esophagus, forming the primordium of mediastinum ,separating the pericardial cavity from the pleural cavities. The primordialmediastinum consists of a mass of mesenchym ( embryonic connective tissue ) that extendes from the sternum to the vertebral column, separating the developing lungs. The right pleuropericardial opening closes earlier than the left one , probably because the right common cardinal vein is larger than the left one, and produces a larger pleuropericardial membrane.
Pleuroperitoneal Membrane As the pleuroperitoneal folds enlarge ,they project into the pericardioperitoneal canals. Gradually ,the folds become membranous.. They are attached dorsolaterally to abdominal wall and their crescentic free edges project into the caudal ends of the canals. During the 6th week these memberanes extend ventromedially until their free edges fuse with the dorsal mesentery of esophagus & septum transversum. This process separates pleural cavities from peritoneal cavity Closure of the pleuroperitoneal openings is assisted by the migration of myoblasts (primordial muscle cells ) into the membranes . The right opening closes before the left one. This may be due to large size of the right lobe of the liver
Development of theDiaphragm 1- septum transversum 2- pleuroperitoneal membranes . 3- Dorsal mesentery of esophagus 4- Muscular ingrowth from lateral body walls Septum Transversum It is first identifiable at the end of the third week as a mass of mesodermal tissue cranial to the pericardial cavity . After head folds at 4th week, it forms a thick incomplete partition between pericardial & abdominal cavities . There is a large opening on each side of the esophagus ( pericardioperitoneal canal ) . This septum is the primordium of the central tendon of the diaphragm. It does not separate the thoracic & abdominal cavities completely. Because there is pericardioperitoneal canal . It expands and fuses with the mesenchyme ventral to esophagus & pleuroperitoneal memberanes
The transverse septum grows dorsally from the ventrolateral body wall and forms a semicircular shelf which separates the heart from the liver . A large part of the liver is embeded in the septum .It is located caudal to the pericardial cavity and partially separates it from the developing peritoneal cavity
PleuroperitonealMemberanes It forms the primordial diaphragm It forms large portion of fetal diaphragm . But they form small portion of the newborn infant’s diaphragm . At the end of the 6th week it fuse with the other 2 components( 9 to 12 ws ) . Dorsal Mesentry of esophagus It forms the median portion of the diaphragm . The crura .( a leglike pair of muscle bundles that cross in the median plane anterior to the aorta . It develop from myoblasts that grow into the dorsal mesentery of esophagus .
muscular ingrowth fromlateral body walls During 10th to 12 th weeks, the lungs and pleural cavities enlarge, into the lateral body walls . During this process the body- wall tissue is split into 2 layers : An external layer that becomes part of the definitive abdominal wall . An internal layer that contributes to peripheral parts of the diaphragm , external to the parts derived from the pleuroperitoneal membranes . As the 4 parts of the diaphragm fuse mesenchyme in the septum transversum extends into the other 3 parts It forms myoblasts that differentiate into the skeletal muscle of the diaphragm .
Positional Changes Durind the 4th week ( A ) & At 6 week it is at the level of the thoracic somites & by the beginning of the 8th week , the dorsal part of the diaphragm lies at the level of the 1st lumbar vertebra Innervation of the diaphragm During the 5th week , myoblasts from 3,4;5 somites migrate into the developing diaphragm ( S. T. ) bringing their nerve fibers with them ( phrenic n. ) which arise from the venteral primary rami of the 3rd, 4th; 5th cervical spinal nerves. The embryonic phrenic ns. Enter the diaphragm by passing through the pleuropericardial membranes . This explain why phrenic ns. Lie on the fibruos pericardium. Hence it is motor to diaphragm and also sensory , but the costal rim receives sensory supply from the lower intercostal ns. Because of the origin of the peripheral part of the diaphragm from the lateral body walls.
Posterolateral defect of the diaphragm is a common congenital anomaly of it . It occurs about once in 2200. Incongenital diaphragmatichernia ,CDH, herniation of stomach, spleen; most of intestines herniate. Usually, unilateral CDH results from devective formation and or fusion of the pleuroperitoneal membrane with other 3 parts of the diaphragm. CDH, occurs on the left side in 85 to 90 % of cases This may be due to earlier closure of the right pleuroperitoneal opening . CDH, is the most common cause of polyhydramnios & pulmonary hypoplasia that because the lug is copressed In severe lung hypoplasia , some primordial alveoli rupture, causing air to enter the pleural cavity , pneumothorax, Also, fetal lung maturation may be delayed. Prenatal diagnosis of CDH: ultrasound& magnetic resonance imaging. It can repair prenatally between 22 & 28 Ws. But there is risk to fetus and mother .