Download

1 / 0
0 likes | 279 Views
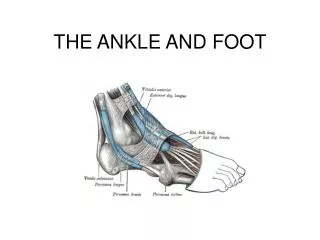
Ankle problems/procedures and techniques. Ankle Arthroscopy. Indications. Diagnostic Treatment Impingement Removal FB Stabilisation OCD’s Fusion procedures. Set up is everything. Mark out important structures like peroneal nerve Think about traction Inflate ankle with saline.

E N D