Download
1 / 43
500 likes | 1.71k Views
The Use of Spinal Orthoses After Spinal Cord Injury. David X. Cifu, M.D. The Herman J. Flax, M.D. Professor and Chairman Department of Physical Medicine and Rehabilitation Virginia Commonwealth University. SCI Rehabilitation Model Systems Project.

E N D
The Use of Spinal Orthoses After Spinal Cord Injury David X. Cifu, M.D. The Herman J. Flax, M.D. Professor and Chairman Department of Physical Medicine and Rehabilitation Virginia Commonwealth University
SCI Rehabilitation Model Systems Project • 16 centers across the United States with uniform admission criteria and rehabilitation care protocols. • More than 20,000 subjects since mid-1970’s. • This research supported by the National Institute on Disability and Rehabilitation Research, Office of Special Education and Rehabilitation and Rehabilitative Services, U.S. Department of Education Grant #H133N50015
Spinal Cord Injury • SCI incidence in the United States is 30 to 40 per million, or 7000-10,000 new cases annually. • While SCI occurs predominantly in individuals aged 16 to 30 (~ 60%), over the past quarter century the age at time of SCI has been rising . • Nearly 20% of new SCI injuries occur in those over 60 years
Spinal Cord Injury • Short term costs range from $100,000 - 1 million. • Lifetime medical costs exceed $1 million/person. • Significant burden on non-medical system (family, vocational, formal support systems)
Spinal Cord Injury • Extensive short and long-term medical issues: • Neurogenic bowel and bladder • Cardiovascular • Pulmonary • Integument (Skin) • Osteoporosis • Pain
Spinal Orthoses: History • Ancient Egyptians used first splints nearly 5,000 years ago, but not to stabilize joints or body parts. • Middle Ages armorers manufactured splints that protected as well as stabilized the body. • French surgeon, Ambroise Pare` developed metal corsets in the late 16th century
Spinal Orthoses: History • Lorenz Heister is credited with developing the first spinal orthosis in the late 17th century. It was quite similar to the modern day Halo brace. • The basic principles of spinal immobilization have actually changed little in the past 300 years, however the materials used and combination of surgery and bracing has changed tremendously.
Spinal Orthoses: Principles • Four objectives of spinal orthoses: • controlling spinal position by external forces • applying corrective forces to abnormal curvatures • providing spinal stabilization when soft tissues cannot • restricting spinal segment movement after trauma
Spinal Orthoses: Principles • Orthoses work through the biomechanical effects of a three-point pressure system on: • trunk and head support • motion control • spinal realignment • partial weight transfer of the head to the trunk when in upright
Spinal Orthoses: Principles • Orthoses effectiveness is affected by: • points of application • direction and magnitude of the forces applied • tightness of the device • type of trauma/injury and the instability produced • body habitus of the individual wearing it
Spinal Orthoses: Principles • Spinal orthoses can also have significant negative effects: • axial muscle atrophy secondary to reduced activity • immobilization can promote contractures • excess pressure, irritation, and moisture build-up can result in skin breakdown • psychological dependency can occur that increases physical dependence • significant functional limitations of orthoses can have untoward psychosocial and economic effects
Cervical Orthoses • To be effective they must control both gross and intersegmental movements of the head and neck. • C0-C1 segment involves significant flexion-extension, minor lateral bending and little rotation. • C1-C2 segment involves primarily rotation (50% of all rotation) with limited flexion-extension. • C3-C7 segments involve flexion extension (C5-C7), lateral bending (C2-C3), and rotation (C2-C3).
Cervical Orthoses • Challenges to immobilization: • extremely mobile joint complex with multiple planes • little body surface available for contact • high incidence of skin breakdown (occiput, chin) • pressure-related pain common (clavicles, chin) • hygiene issues limit comfort (shaving) • Opportunities: • strong interest in pre-hospital immobilization systems • $40-million/year market
Cervical Orthoses: Collars • Cervical collars [25-100% normal motion] • soft/foam - inexpensive and comfortable; no immobilization; provides warmth and psychological support; primarily serves as a reminder; 75-100% normal motion • hard/rigid - mildly limits flexion/extension if optional occipital/mandibular struts in place; no limitation of lateral bending or rotation; painful at clavicles • Philadelphia - significantly limits flexion/extension primarily; 25-30% normal motion uncomfortable at clavicles; • Other - Jobst Vertebrace, Miami J, Aspen/Newport, NecLoc may be slightly superior to Philadelphia
Cervical Orthoses: Posters • Poster Appliances: [10-28% normal motion] • Four poster - mandibular/occipital supports with struts to anterior/posterior thoracic plates; excellent limitation of flexion/extension. • Guilford/Two Poster - similar to four poster with addition of axilla straps and thoracic belt.
Cervical Orthoses: CTO’s • Cervicothoracic Orthoses: [10-25% normal motion] • Yale - Combination of a high Philadelphia collar with thoracic jacket and axillary straps; Excellent flexion/ extension control; Fair rotation control • SubOccipital Mandibular Immobilizer (SOMI) - Similar to four poster with crisscrossing full thoracic body jacket; removable head strap to allow mandibular support to be removed with eating; may be applied w/o turning patient; comfortable; Fair restriction of flexion/extension only
Cervical Orthoses: Halos and Beyond • Halo devices: [10-25% normal motion] • Halo Vest - metal/graphite ring attached to the skull in 4 points affixed to full thoracic vest by 4 posters; Excellent control of all motions • Halo Cast - similar to vest except cast is fabricated to get improved purchase • Thermoplastic Minerva Body Jacket (TMBJ): • improvement over casted version (lighter); may be as effective as Halo vest; non-invasive (no pins)
Cervical Orthoses: Utility • Orthoses do not achieve total or near total immobility. Overall fit quite variable and will change with usage. • In the face of neurological deficit, non-surgical patients require 3+ months orthosis. • When good anatomic alignment can be achieved, need for surgery is unclear. • Non-surgery patients have better long-term ROM. • Surgical patients require 6+ weeks orthosis.
Cervical Orthoses: Utility • Higher cervical injuries are better immobilized. • Individuals with injuries to the facet joints (dislocation +/- fracture) are most likely to need surgery. • A patient who is unstable at 6 weeks (post-surgery) or 12 weeks (non-surgical) despite orthosis use will need later surgery (although “instability” is not necessary absolute indication). • Rapid mobilization achieved with either method.
ThoracoLumbar Orthoses • More commonly prescribed than cervical orthoses. • Similar immobilization issues as in cervical region. Sacrum is the foundation of the spine. • Actual control of motion poorly studied. • Extensive research on the usage of TLO’s (variable types) in the prevention of injuries has not demonstrated any reduction in stresses to the spine, muscles, or abdominal contents with these devices.
ThoracoLumbar Orthoses • Thoracic Motion: • horizontally-oriented facets and ribcage attachments to sternum limit flexion/extension, exc. In lower region. • 6-9 degrees of lateral bending and rotation in each segment. • Lumbar motion: • Predominant motion is flexion/extension, followed by lateral bending and then rotation. • Greatest flexion/extension and least bending/rotation at L5-S1.
Lumbosacral Orthoses: Types • Lumbosacral Orthoses: • Chairback brace - anterior corset/apron with midaxillary metal uprights; controls flexion extension • William’s brace - allows free flexion and limits extension; uses lever action and abdominal support to decrease lordosis
ThoracoLumbar Orthoses: Types • Thoracolumbar Orthoses (TLSO’s): • Taylor brace - Thoracolumbar corset with axillary straps; designed to limit flexion/extension; Poor efficacy • Molded jackets - thermoplastic or casted; highest efficacy to control post-fracture/injury spinal motion • Jewett Hyperextension brace - three-point pressure over sternum, pubis and posterior lumbar spine; prevents flexion; used with compression fractures; not indicated with osteoporosis secondary to excess forces generated
Thoracolumbar Orthoses: Utility • Orthoses do not achieve total or near total immobility. Overall fit quite variable and will change with usage. • In the face of neurological deficit, surgery is typically performed. • Even when good anatomic alignment can be achieved, surgery is often needed. • Non-surgery patients have better long-term ROM. • Surgical patients require 6+ weeks orthosis.
Thoracolumbar Orthoses: Utility • Thoracic injuries are better immobilized than lumbar. • Individuals with significant ligamentous injury and instability are most likely to need surgery. • A patient who is unstable at 6 weeks (post-surgery) or 12 weeks (non-surgical) despite orthosis use will need later surgery (although “instability” is not necessary absolute indication). • Rapid mobilization best achieved with surgery.
Summary • SCI’s are an infrequent but potentially devastating injury that greatly stress healthcare and psychosocial resources. • Integrated systems of care are necessary to optimally manage care after SCI. • Rapid and safe mobilization with surgery and orthoses is key to efficient and successful rehabilitation. • Initial and long-term orthosis fitting is crucial.
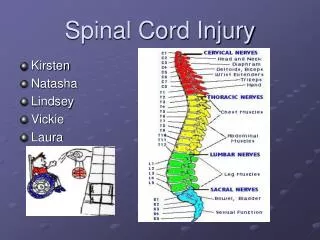
SCI Classification • ASIA Classification identifies lowest level of normal function (C1 - S5) and degree of completeness: • A - Motor and Sensory Complete • B - Motor Complete • C - Motor Incomplete but non-functional • D - Motor Incomplete, functional • E - Recovery of Neurologic Function
SCI Classification • Tetraplegia - Arms and Legs involved (C1-7) • Paraplegia - Trunk and Legs involved (T1-S5) • Central Cord - Arms predominantly involved • Brown Sequard - Motor weakness on one side of body and sensation deficits on other • Cauda Equina - Predominant bowel and bladder deficits with mild leg weakness
SCI: Common Issues • Spinal Stability • Pulmonary • Neurogenic Bowel and Bladder • Immobility: Skin Breakdown/DVT • Spasticity • Autonomic Dysreflexia/Cardiovascular • Bracing/Equipment • Heterotopic Ossification • Pain
SCI: Spinal Stability • Stabilizing the spine is necessary before mobilization to prevent worsened injury and decrease pain. • Surgery has not been specifically demonstrated as superior to bracing, but typically performed. May allow earlier mobilization. • Spinal bracing often present for 6-12 weeks. Uncomfortable and difficult to maintain.
SCI: Pulmonary • Pulmonary compromise is common with injuries involving the cervical region. Diaphragm innervated from C3-5. Also, muscles of chest wall and abdomen are needed for optimal breathing. • Individuals with C4 injuries (motor complete) and above may require lifetime ventilation. Newer techniques are improving this. • Higher short and long-term incidence of pneumonia in individuals with cervical injuries.
SCI: Neurogenic B/B • Control of Bowel and Bladder function maintained at 3 levels: • Frontal Cortex: Social control; empty at set volumes • Pontine: Hyperreflexic B/B; may empty partially, need assistance with full (intermittent catheterization, bowel program) • Lumbar: Hyporeflexic B/B; Bladder and Rectum are like flaccid sacs, emptying occurs with excess volumes; Good control challenging
SCI: Sexuality • Sexuality entails much more than the waterworks, however challenging for younger individuals to get beyond it. • Cervical and thoracic injuries are more likely to have reflex erectile function (rarely enough to achieve penetration/ejaculation). • Lumbar and sacral injuries rarely demonstrate erectile function. • Interventions range from Viagra to Pneumatic devices. Electroejaculation available.
SCI: DVT • Deep venous thromboses are blood clots in the venous system related to vessel wall trauma, hypercoagulability from trauma, and immobility. • Occur in 40-60% of SCI’s. Most common cause of late death. Often asymptomatic acutely. Cause chronic edema and pain. • Prophylaxis with anticoagulant is effective and needed for 8-12 weeks. • Treatment with anticoagulant is necessary for 3-6 months.
SCI: Skin Breakdown • Due to the inability of individuals with SCI to move/turn in bed and chairs, excess skin pressures occur rapidly. Skin breakdown occurs within 2 hours of immobility. • Decreased sensation limits patient input. • Initially, repositioning every 2 hours is needed. • Skin ulcers are common and take weeks to months to heal ($25,000 each). Healing occurs with preventing pressure and keeping area clean/dry.
SCI: Spasticity • Any upper motor neuron (brain/spinal cord) injury can result in an imbalance of excitatory to inhibitory neurotransmitter release to muscles. • Spasticity is increased, velocity dependent resistance to stretch in muscle groups. • Limits motion of joints and utility of preserved muscle strength, may be painful, may cause falls or functional deficits. On the other hand, may maintain muscle bulk, decrease pressure ulcers, and prevent DVT’s.
SCI: Spasticity • In many patient, spasticity improves over first 3-6 months. • Treatment initially entails decreasing irritant foci that may potentiate (full bladder, pressure ulcer, ingrown toenail, tight fitting garments) • Treatment also entails stretching, positioning, and desensitizing extremities. • Numerous systemic (Baclofen, Dantrium) and focal (Botox, Myobloc) medications that are effective.
SCI: Autonomic Dysreflexia • In individuals with SCI above T6 level, there is a disconnect between the sympathetic and parasympathetic autonomic nervous systems. • Stimuli of parasympathetics may set off unblocked sympathetic response resulting in elevated BP and headache. Can result in stroke/death if untreated. • All individuals with SCI experience significant cardiovascular deconditioning over time, accelerated compared to non-SCI. Close medical f/u and encouraging aerobic exercise is vital.
SCI: Bracing • Extensive assortment of arm and leg orthoses to stabilize joints, substitute for weak muscles, and facilitate function. • Upper extremity devices to achieve various types of gripping and holding for C7 and higher individuals are commonly used long-term. • Lower extremity braces that allow functional transfers or walking, without the assist of another, are also commonly used long-term.
SCI: Wheelchairs • Individuals with C6 and below SCI can independently propel W/C’s. Electric W/C’s are common above. • Lightweight (20 lbs) chairs are typical for functional mobilizers. • Individuals with C5 and below can commonly operate motor vehicles (with/without modifications).
SCI: Heterotopic Ossification • Abnormal deposition of calcium in muscle or around joints in the first 4-12 weeks post-injury. • Unclear etiology, although traumatized joints and muscle at highest risk. • Symptoms include pain, swelling, and redness. Occurs below the level of the lesion. • Treatment is early identification to facilitate rapid mobilization and medication management.
SCI: Pain • Pain is common symptom following trauma of SCI as well as neurologic disruption. • Soft tissue pain usually improved by 6 weeks. • Neuropathic pain common at “zone of injury”. Challenging to treat, often undertreated. Medications include antiepileptics (Tegretol, Neurontin), tricyclic antidepressants (Elavil), antiinflammatories, narcotics, local patches (Lidocaine) and liniments (Capsaisin).