Download

1 / 30
850 likes | 2.7k Views
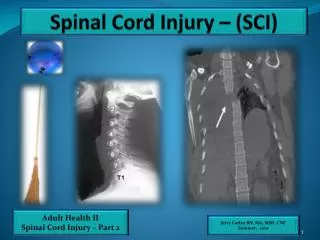
Spinal Cord Injury. (SCI). SCI Epidemiology. Incidence: 11,000 new cases per year. Prevalence: 225,000-296,000 persons in the USA living with SCI. Traumatic SCI is most common in people aged 16-30 (more than 50% of cases). Most common cause of traumatic SCI: Motor vehicle accidents – 47%

E N D
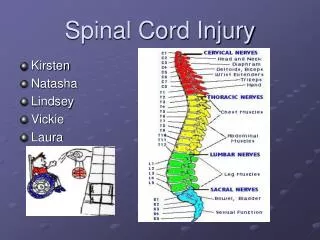
Spinal Cord Injury (SCI)
SCI Epidemiology • Incidence: 11,000 new cases per year. • Prevalence: 225,000-296,000 persons in the USA living with SCI. • Traumatic SCI is most common in people aged 16-30 (more than 50% of cases). • Most common cause of traumatic SCI: • Motor vehicle accidents – 47% • Falls – 23% • Violence (esp. gunshot wounds) – 14% • Sports accidents – 9% • Other – 7% • 78% male, 63% Caucasian.
48% paraplegic and 52% tetraplegic, 52% incomplete and 48% complete. • Life expectancy for paraplegics (in those who live for one year) is near normal. • Life expectancy for tetraplegics is reduced by ~10 years (reduced by ~20 years if ventilator dependent).
Spinal Cord Anatomy http://www.brianjogrady.com/neurosurgery.html
Types of Injury • Upper motor neuron injury: injury to the neurons in the brain and/or spinal cord. – Increased tone, brisk reflexes. – Involuntary spasms, preserved muscle bulk. – Occurs in brain injury and SCI down to the conus medularis – (So, fractures above L1 usually give upper motor neuron picture).
Types of Injury • Lower motor neuron injury: injury to the nerves after they synapse in the spinal cord. – Decreased muscle tone – Areflexic – Muscle atrophy – Incontinent of bowel/bladder – 4% of patients with SCI above L1 are LMN injuries.
Spinal Cord Tracts • Corticospinal: descending tracts (also called the pyramidal tracts). – Motor control. • Spinothalamic: Ascending tracts. – Pain and temperature. • Dorsal columns: ascending (also called the posterior columns). – Vibration, proprioception, and light touch. http://img.orthobullets.com/Spine/Introduction/Electrophysiologic%20Monitoring/Images/Pathways.jpg
Central Cord Syndrome- – Occurs with cervical level injuries. – Typically results in greater weakness in upper limbs than lower. – Bowel/bladder usually preserved. • Brown-Sequard Syndrome - Results from hemisection). – Ipsilateral loss of motor function, light touch, vibration, and proprioception. – Contralateral loss of pain and temperature sense. http://img.tfd.com/mk/C/X2604-C-28.png http://img.tfd.com/mk/B/X2604-B-40.png
Anterior cord syndrome – usually vascular cause from damage to the anterior spinal artery. – Loss of motor function (with spasticity). – Loss of pain and temperature sense. – Some loss of light touch. – Vibration and proprioception are preserved. – Poor prognosis for motor recovery. http://img.tfd.com/mk/A/X2604-A-47.png
Blood Supply to Cord http://www.frca.co.uk/images/spinal-cord4.jpg
Posterior Cord Syndrome – damage to dorsal columns. – Loss of vibration and proprioception. – Can see spastic weakness and bladder dysfunction. – Causes include trauma, B12 deficiency. http://www.stepahead.org.au/media/images/posterior-injury.jpg
Conus medullaris: the end of the spinal cord, contains the sacral reflex center. – Weakness in lower limbs. – Areflexic bowel and bladder (sometimes with preserved reflexes) • Cauda Equina: “Horse’s Tail” lumbosacral nerve roots within the spinal canal. – Areflexic bowel, bladder, and lower limbs. – “Saddle Horse” Anesthesia http://img.tfd.com/mk/C/X2604-C-23.png http://www.aceproindia.com/ACE%20Sample%20Projects/ePUB/Examination%20and%20Diagnosis%20of%20Musculoskeletal%20Disorders/OEBPS/images/9783131605818_c008_f048.jpg
Acute Events s/p SCI • First few hours patients experience neurogenic shock due to interruption of sympathetic nervous system to regions below the cord injury, and subsequent vasodilation • Triad of: bradycardia, hypotension, and hypothermia • ASIA Exam at this time is not prognostic due to other possible injuries present and neurogenic shock (must wait at least 72 hours to evaluate)
Transient Paralysis/Spinal Shock • Loss of all physiological functioning caudal to the cord injury • Flaccid paralysis, anesthesia, absent bowel and bladder control, loss of reflexes • Some males may experience priaprism after cervical injuries • May last hours to weeks • Early return of DTRs is associated with better prognosis • Exact pathophysiology is not well understood, it is thought to be related to the release of K+ by the injured cells in the cord leading to an accumulation of extracellular K+ that eventually normalizes and results in resolution of the spinal shock • As spinal shock resolves spasticity becomes evident
Medical Management • Cardiovascular • Autonomic dysregulation results in Triad of: Hypotension, Bradycardia, and Hypothermia • Must maintain BP for adequate perfusion to the injured cord using fluids, pressors, and transfusions initially • Monitor electrolyte levels, urinary output, and fluid administration • Autonomic Dysreflexia (AD): usually occurs later • Headache, flushing, episodic paroxysmal HTN, bradycardia, and sweating • Pain is often the cause of this phenomenon
Pulmonary • Initially High Risk of:PE, respiratory failure, pulmonary edema, pneumonia • Highest incidence of the above with cervical lesions • Decreased strength of diaphragm and chest wall muscles leads to difficulty of clearing secretions, ineffective cough, and hypoventilation • Frequent suctioning and chest physiotherapy should be implemented ASAP • In respiratory failure intubation and ventilation required • Pneumonia is the leading cause of death at any point s/p SCI
DVT/PE • Occurs in 50-100% of untreated patients • Most common in first 72 hours to 14 days • All pts should receive DVT prophylaxis • Treatment of choice: Low-molecular-weight heparin with compression stockings • IVC filters required in patients when anticoagulation is contraindicated • Skin • Impaired autoregulation of skin capillaries and decreased sensation increases risk of skin breakdown • Pressure sores develop quickly, especially on heels and buttocks • Patients should be rolled q 2 hours • Special rotating beds are also used for prevention • Multipodus boots protect heels
Neurogenic Bladder • Detrusor-sphincter dyssynergia (DSD) • Lack of sphincter relaxation during bladder contraction • Results in urinary retention and vesicoureteral reflux • Treatment: • Intermittent catheterization • Oral or intravesicular anticholinergics • Alpha blockers • Stent placement • Sphincter botulinum injections • neurostimulation
Neurogenic Bowel • Loss of bowel reflexive function results in ileus • Treatment: • Stool softeners (Colace), rectal stimulant (Ducolax), and colonic stimulant (Senna) • Goal is to create a bowel regiment that allows for control of the timing of bowel emptying
Heterotropic Ossification • Formation of bone in soft tissue adjacent to neurologically affected joints • Metaplasia of mesenchymal cells into osteoblasts • More commonly seen near large joints • Usually 1-4 months post injury • Symps: swelling, decreased ROM, warmth, spasticity • Plain X-ray or Triple-Phase Bone Scan used for diagnosis • Treatment: • joint rest, ice, gentle ROM exercises • NSAIDS (indomethacine) • Bisphosphonates • Etidronate (also used preventatively) • reduces osteoblast/clast activity and calcium phosphate precipitation • Surgical resection
Heterotropic Ossification http://www.physio-pedia.com/images/1/11/Ho1.jpg
Sexual Fuction/Fertility • ED is more common acutely after SCI, but resolves with time. Many men are able to maintain an erection suitable for sexual activity • LMN injury – lack of erection • UMN injury – reflexogenic erection • Fertility may be reduced in males who have retrograde ejaculation or impaired spermatogenesis • Fertility in females is uncompromised, however, labor maybe difficult due to lack of voluntary muscle control • Uterine contractions are present
Glucocorticoids – Methylprednisolone • Limited evidence (mainly animal studies) have shown that when given in first 8 hours after SCI, better outcomes are achieved • May reduce edema, intracellular K+ depletion, and improve neurologic recovery • Timing is crucial: late administration may actually interfere with the initial healing process
ASIA Exam http://www.emergency-medicine-tutorials.org/_/rsrc/1257199993383/Home/surgical/trauma/spinal/neuro-exam-chart/Spinal%20neuro%20exam%20chart.JPG
Level Terminology • Neurological Level: The unifying level to describe the overall fxn. It combines sensory and motor levels, based on the last level of the cord that is normal. • For C1-C4 and T2-L1 use the sensory level to define the neurological level • Complete Injury: No sensory or motor fxn preserved below the neurological level • Incomplete Injury: If any sensory fxn and/or motor fxn below the neurological level
ASIA Impairment Scale • ASIA A: Complete (no motor or sensory) • ASIA B: Incomplete sensory, but no motor fxn • ASIA C: Motor and sensory fxn Incomplete, with strength of more than half of the key muscles below the level having a muscle grade < 3 • ASIA D: Motor and sensory fxn incomplete, with at least half of the key muscles below the level having a muscle grade > 3 • ASIA E: Normal motor and sensory fxn
ASIA Exam at 72 hours predicts short-term prognosis (2-3 months) • ASIA Exam at 1 month predicts long-term prognosis (1 year) http://www.streetsie.com/wp-content/uploads/paralympic-games.jpg
Expected Functional Levels • C1-3: Ventilator dependent • C5: Can feed self with adaptive equipment • C6: Highest level of complete injury consistent with independent living without aid. Tendonesis orthosis (aids in grasp) and short opponens orthosis with utensil slots. Can drive adaptive van. • C7/C8: Completely independent from a wheelchair level • L2/L3: Gait becomes functional http://www.healthmegamall.com/ProdImages/NCM-NC99485L_lg.jpg
Works Cited • Dawodu, S. T. Spinal cord injury – definition, epidemiology, pathophysiology. (2011, Nov 10) Medscape Reference. Retreived from http://emedicine.medscape.com/article/322480-overview#a30 • Hansebout, R.R., Kachur, E. Acute Traumatic spinal cord injury. In: UpToDate, Aminoff, M.J., Marx, J.A.(Ed), UpToDate, Waltham, MA, 2012. • Ho, C.H., Wuermser, L., Priebe, M., Chiodo, A.E., Scelza, W.M., Kirshblum S.C. Spinal Cord Injury Medicine. 1. Epidemiology and Classification. Spinal Cord Injury Medicine, 2007; 88(3):S49-54. • Choi, H., Sugar, R., David, E.F., Shatzer, M., Krabak, B.(2003). Spinal Chord Injury (SCI). In R. Hurley, E. Wolfberg, C. Sahl (Eds.), Physical Medicine and Rehabilitation Poketpedia (pp. 97-102). Philadelphia; Lippincott Williams & Wilkins.
Kelbine, P., Lindsey, L. (2007, May). Spinal Cord Injury Information Network. Retrieved fromhttp://www.spinalcord.uab.edu/show.asp?durki=22405 • Stiens, S., Goldstein, B., Hammond, M., Little, J. (2008).Spinal Chord Injury Medicine: Acute Treatment, Rehabilitation, and Preventative Care. In J. Merritt, & S. Ward(Eds.), Physical Medicine and Rehabilitation Secrets (pp. 456-465). Philadelphia; Mosby Elsevier.