Download
1 / 13
130 likes | 241 Views
MTEV en Réanimation. Neuhaus 1978 Décompensation respiratoire EP autopsie 27 % Hirsh 1995 Dec Resp, H digestive, Dec Cardiaque, Sepsis écho-doppler veineux 2x/sem + 1sem après sortie réa TVP 33% TVP distale 12 % TVP proximale 16 %

E N D
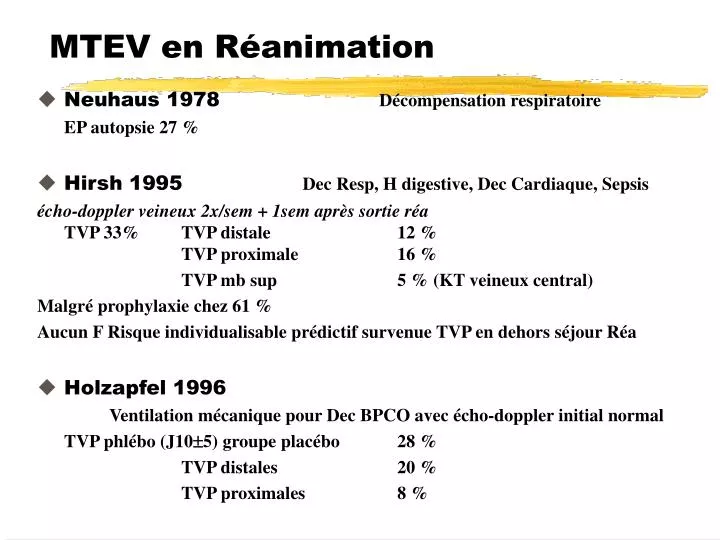
MTEV en Réanimation • Neuhaus 1978 Décompensation respiratoire • EP autopsie 27 % • Hirsh 1995 Dec Resp, H digestive, Dec Cardiaque, Sepsis • écho-doppler veineux 2x/sem + 1sem après sortie réa • TVP 33% TVP distale 12 % • TVP proximale 16 % • TVP mb sup 5 % (KT veineux central) • Malgré prophylaxie chez 61 % • Aucun F Risque individualisable prédictif survenue TVP en dehors séjour Réa • Holzapfel 1996 • Ventilation mécanique pour Dec BPCO avec écho-doppler initial normal • TVP phlébo (J105) groupe placébo 28 % • TVP distales 20 % • TVP proximales 8 %
MTEV en Réanimation • Neuhaus 1978 Décompensation respiratoire • EP autopsie 27 % • Hirsh 1995 Dec Resp, H digestive, Dec Cardiaque, Sepsis • écho-doppler veineux 2x/sem + 1sem après sortie réa • TVP 33% TVP distale 12 % • TVP proximale 16 % • TVP mb sup 5 % (KT veineux central) • Malgré prophylaxie chez 61 % • Aucun F Risque individualisable prédictif survenue TVP en dehors séjour Réa • Holzapfel 1996 • Ventilation mécanique pour Dec BPCO avec écho-doppler initial normal • TVP phlébo (J105) groupe placébo 28 % • TVP distales 20 % • TVP proximales 8 %
Prévention MTEV en réanimation médicaleNadroparine • Ventilation mécanique pour Dec resp aiguë BPCO • avec écho-doppler initial normal N = 223 • Nadroparine 0,4 ml / j si < 70 kg Placebo • 0,6 ml / j si > 70 kg • n = 109 n = 114 • délai 24 h - durée 10 ± 5j • âge 69,4 ± 7,7 ans p=0,02 66,8 ± 8,2 ans • TVP phlébo 12/84 14%p=0,03 24/86 28% • TVP distales 11% 20% • TVP proximales 3 % 8 % • Hémorragies 5 % 8 % • Holzapfel L Am J Respiratory Critical Care Med 1996;153:Abstract A96
Anticoagulants à la phase aiguë AVC ischémique • rec avc hémor ic décès ou évolution décès ou (N ) isch avc hémor avc non fatal favorable dépendance • IST 1997 • délai 48h pour14J J14 J14 J14 • sans héparine (9717) 3,8%** 0,4%**** 12,0% • héparine (9716) 2,9%** 1,2%**** 11,7% • TOAST 1998 • délai 24h pour7J J10 J10 3 mois 3 mois • placebo (634) 1,5% 0,8%* 12,4% 74% 55%* (117) • Danaparoïde (641) 1,7% 2,3%* 12,6% 75% 68%* (113) • athérosclérose carotidienne • FISS 1995 • délai 48h pour10J J10 J10 6 mois 6 mois • placebo (105) 4,8% 9,5% 19,1% 65%*** • Nadroparine 4100U/j (101) 2,0% 6,9% 16,8% 52% • Nadroparine 8200U/j (102) 1,0% 4,9% 13,0% 45%*** • FISS bis : échec • p 0,05*, p<0,01**, p<0,005***, p<0,00001**** del Zoppo G 1999
Prévention MTEV lors AVC ischémique • Essais TVP / N patients incidence TVP [IC 95%] RRR • Contrôles 4 161 / 257 63% [ 57 - 69 %] • HNF faible dose 2 47 / 202 23% [ 17 - 29 %] - 63% • HBPM 4 27 / 167 16% [ 10 - 22 %] - 75% • Clagett ACCP 1998
Prévention MTEV lors AVC ischémique • Essais TVP / N patients incidence TVP [IC 95%] RRR • Contrôles 4 161 / 257 63% [ 57 - 69 %] • HNF faible dose 2 47 / 202 23% [ 17 - 29 %] - 63% • HBPM 4 27 / 167 16% [ 10 - 22 %] - 75% • Clagett ACCP 1998
Prévention MTEV lors AVC ischémique • Essais TVP / N patients incidence TVP [IC 95%] RRR • Contrôles 4 161 / 257 63% [ 57 - 69 %] • HNF faible dose 2 47 / 202 23% [ 17 - 29 %] - 63% • HBPM 4 27 / 167 16% [ 10 - 22 %] - 75% • Clagett ACCP 1998
IST 97, TOAST 98 : EP symptomatiques • IST 1997 EP symptomatique (fatale ou non) J14 • héparine 9716 0,5% p<0,05 • sans héparine 9717 0,8% • aspirine 9719 0,6% p=0,08 NS • sans aspirine 9714 0,8% • IST group Lancet 1997;349:1569-1581 • TOAST 1998 TVP sympto 3 mois EP sympto 3 mois • Danaparoïde 638 0,3% p<0,05 0,3% • placebo 628 1,6% 0,6% • TOAST JAMA 1998;279:1265-1272
Anticoagulants à la phase aiguë AVC ischémique : IST 97 • Évènements J14 Thrombo-Embolies Hémorragies Total • (N) EP sympto + réc AVC isch H maj + H intra-cran sympto • Aucun traitement 0,9% + 4,4% = 5,3% 0,3% + 0,3% = 0,6% 5,9% • (4859) • Aspirine 300 mg/j 0,7% + 3,2% = 3,9% 0,5% + 0,5% = 1,0% 4,9% • (4858) • HNF 10000 U/j 0,8% + 3,2% = 4,0% 0,4% + 0,7% = 1,1% 5,1% • (2429) • HNF 10000 U/j + 0,5% + 2,1% = 2,6% 0,8% + 0,8% = 1,6%4,2% • Asp 300mg/j (2431) • HNF 25000 U/j 0,5% + 3,5% = 4,0% 1,4% + 1,8% = 3,2% 7,2% • (2426) • HNF 25000 U/j + 0,3% + 2,8% = 3,1% 2,7% + 1,7% = 4,4% 7,5% • Asp 300mg/j (2430) • IST group Lancet 1997;349:1569-1581
Prévention MTEV lors AVC ischémique:Enoxaparine • AVC ischémique athérothrombotique avec parésie Mb Inf • sans infarctus hémorragique au scanner • Enoxaparine 40 mg / j HNF 5000 U 3x/j • 8 -12 j, 10 ± 2 j • TEV 15 / 76 19,7% p = 0,04425 / 72 34,7% • TVP (phlébo) • EP (scinti ou angio) • autopsie • Infarctus hémorragique • 14 / 81 17,3% 20 / 86 23,3% • Critère combiné 31 / 80 38,8% 40 / 78 51,3% • TVP, EP, décès, • hémorragies intra-crâniennes, infarctus hémorragiques, hémorragies majeures • Hillbom ISTH, ASH 1999
MTEV en Neurochirurgie : Epidémiologie • TVP *Fg contrôles 19 à 50% • TVP phlébo contention veineuse 24 à 33% • EP autopsie 25 % • EP cause primaire de décès dans 50% des cas • TVP EP symptomatique 4% • Facteurs de risque • Chirurgie intra-crânienne > rachis • Tumeur maligne > bénigne • sus-tentorielle • Gliome malin = Méningiome • Durée chirurgie • Parésie ou paralysie Mb Inf • Agnelli 1999
Prévention MTEV en neurochirurgie (1) • Compression pneumatique intermittente = Contention veineuse • TEV 23% 6% RRR : - 74% • insuffisant chez sujet à haut risque : tumeur cérébrale ou médullaire • HNF dose fixe • Cerrato 1978 (n=100) HNF 5000U 3x/j versus contrôles • TVP *Fg 6% 34% RRR: -82% • Bostrom 1986 HNF 5000U 2x/j versus stim électrique + Dextran • TVP *Fg 10% 13%
Prévention MTEV en neurochirurgie (2) • TVP phlébo J7 J10 Hémorragies • n évaluables Ttt contrôle n Ttt Contrôles • Melon 1987 • Enoxaparine 20mg/j 18-24 h post-op versus placebo • 122 15,6% 24,1% 130 0% 0% • Nurmohamed 1996 • contention + Nadroparine 7500U/j 18-24h post-op versus contention • 345 18,7% 26,3% 130 4,1% 1,2% • Agnelli 1998 • contention + Enoxaparine 40mg/j 24 h post-op versus contention • 260 16,9% 33,1% 307 11,8% 7,1% • Total surtout hémorragies intra-crâniennes • 727 17,5% 28,3% 922 6,1% 3% • RRR: -38%ARR: +100% • Agnelli 1999