Download
1 / 26
480 likes | 2.71k Views
Acute Poststreptococcal Glomerulonephritis. MR 7/27/09 J. Chen. Outline. Background Pathophysiology Histologic Findings Clinical History Physical Lab Differential Diagnosis Treatment Follow Up. Background.

E N D
Acute PoststreptococcalGlomerulonephritis MR 7/27/09 J. Chen
Outline • Background • Pathophysiology • Histologic Findings • Clinical • History • Physical • Lab • Differential Diagnosis • Treatment • Follow Up
Background • Glomerulonephritis-various renal diseases in which inflammation of the glomerulus, manifested by proliferation of cellular elements, is secondary to an immunologic mechanism • Most associated with postinfectious state • 4-12yr with peak 5-6years • Male:Female 1.7-2:1 • Prognosis is good
Winter and Spring-respiratory infection • Latency period 10 days for pharyngitis • Summer and Fall-associated with pyoderma • Latent period difficult to determine
Pathophysiology • Not fully understood • Immune Complexes localize on glomerular capillary wall and activate the complement system (Zymogen and GAPDH) • Activation of complement cascade generates C5a and platelet derived inflammatory mediators • Various cytokines initiate an inflammatory response manifested by cellular proliferation and edema of glomerular tuft
Membrane attack complex (C4bC2a) (C4 + C2) Recruitment of PMNs C3b C3 C3a Opsonization, phagocytosis C3 convertase Alternative pathway Anaphylaxis, Chemotaxis Microbial surfaces (polysaccharides) Complement Abnormalities Ab-Ag complexes C3 convertase Classical pathway
Measurable reduction in volume of glomerular filtrate • Decreased capacity to excrete salt and water leading to expansion of extracellular fluid volume • Responsible for edema and in part for hypertension, anemia, circulatory congestion, encephalopathy
Histologic Findings • Light Microscopy-Glomerular tufts enlarged and swollen
Electron Microscopy of renal tissue • Electron-dense deposits (humps) in the subepithelial space
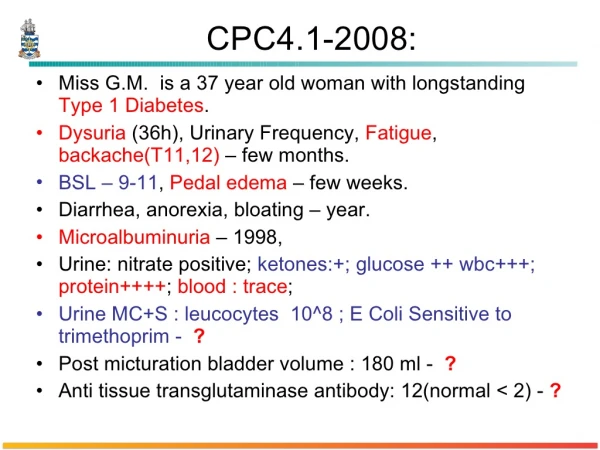
Clinical Presentation • History: latent period 7-21 days btw streptococcal infection and glomerulonephritis characteristics • Edema most frequent manifesting symptom • 85% • Abrupt onset • Periorbital area, may be generalized • Gross hematuria 30-50% • Smoky, cola, rust, tea colored • +/- oliguria • Various degree of malaise, lethargy, anorexia, fever, abdominal pain, headache
History Continued • Hypertensive encephalopathy-HA, vomitting, depressed sensorium, confusion, visual disturbances, aphasia, memory loss, convulsions, coma • Possible dyspnea, orthopnea, cough • Pallor
Physical • Edema • Systolic and Diastolic HTN to varying degree (Inc ECF, cytokines with pressor effects) • Pallor • Pulmonary rales • Bradycardia/tachycardia • Depressed sensorium
Lab Studies • Urine-output reduced, concentrated, acidic • Hematuria • Proteinuria • Glucosuria • RBC Casts-60-85% • Hyaline and/or cellular casts
Lab Studies Cont • Renal: • Elevation of BUN/Cr usually modest • Electrolytes usually normal (hyperK and met acid with significant renal impairment)
Labs • Streptococcal infection: • Culture from Pharynx and skin may be positive • Strep ab titers more meaningful • Measured at 2-3 wk intervals-Rise more significant
Labs • Hemolytic Complement • C3 decreased in 90% • C4 normal • C5 decreased • Complement levels return to normal 6-8 weeks after onset
Labs • Mild Anemia-parallels the degree of ECF expansion • WBC-Nl • Plts-Nl
Imaging • Renal US-nl to slightly enlarged kidneys • CXR-Central venous congestion • Occasionally enlarged cardiac shadow
Differential Diagnosis • Normal complement • HUS • IgA Nephropathy • HSP • Alport’s / TBMD • Nephrotic Syndrome Hypocomplementemia • PIGN • Bacteria (GAS, S. viridans, pneumococcus, S. aureus, S. epi, atypical mycobacterium, meningococcus, Brucella, Leptospirosis, Propionibacterium) • Viruses (VZV, EBV, CMV, rubeola) • Parasites (Toxo, Trich, Riskettsia) • Membranoproliferative GN • SLE • Cryoglobulinemia • Bacterial Endocarditis • Shunt nephritis
Hematuria Myoglobin Hemaglobin Bile Urate Crystals Beets Blackberry Food dye Drugs Exercise PIGN IGAN Benign Familial Glomerulonephritis MPGN HSP SLE Alport Pyelonephritis Hypercalciuria Nephrolithiasis Trauma Sickle Cell NSAIDS Renal V. Thrombosis Cystitis MeatalStenosis Urethritis Bladder tumor Menstrual contamination Diaper rash
Proteinuria • Nephrotic Syndromes • Acquired Glomerular Disease • MPGN • SLE • IGAN • SBE • DM • HTN • HUS • Genetic Disorders • Nail-patella syndrome • Alport syndrome • Fabry Disease • Glycogen storage disease • CF • Hurler • Gaucher Disease • Wilson Disease • SC • Leukemia • Lymphoma • Infectious • PSGN • HIV nephropathy • HEP B and C • Malaria • Syphilis • Pyelonephritis • Drugs/toxins
Management • Treatment mainly supportive • Hospitalization indicated if:significant HTN, Oliguria, Generalized Edema, High Cr or K • Antibiotics do not influence course of disease-however, administered to ensure eradication of disease
Fluid Restriction • Salt Restriction • Loop Diuretics • Antihypertensives • Limited activity • Dialysis if necessary
Follow Up • Prognosis usually excellent • 0.5% mortality due to pulmonary edema or pneumonia • <1% progress to CKD stage 5 • Follow-up • Must ensure that HTN controlled, Edema resolved, hematuria/ proteinuria resolved, Cr normalized • Gross hematuria resolves within 2 weeks • Complement low for 6-8 weeks • Proteinuria remains upto 6 months • Hematuria remains upto 2 years