Download
1 / 4
40 likes | 229 Views
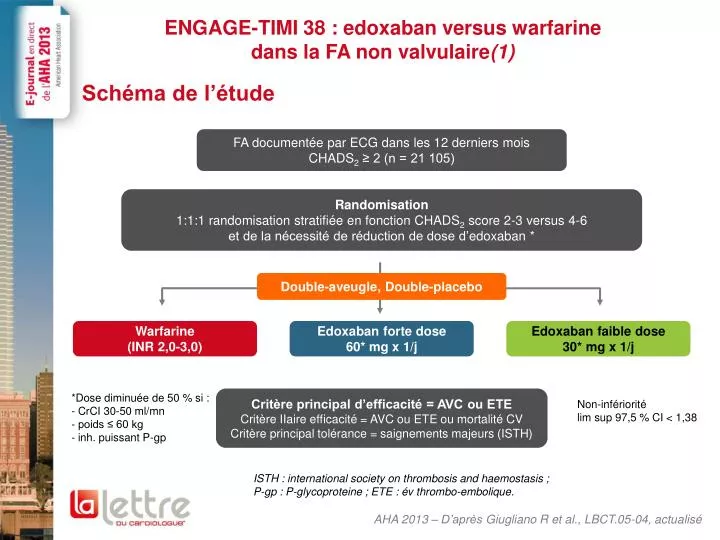
ENGAGE-TIMI 38 : edoxaban versus warfarine dans la FA non valvulaire (1). Schéma de l’étude. AHA 2013 – D’après Giugliano R et al., LBCT.05-04, actualisé. FA documentée par ECG dans les 12 derniers mois CHADS 2 ≥ 2 (n = 21 105).

E N D
ENGAGE-TIMI 38 : edoxaban versus warfarinedans la FA non valvulaire(1) Schéma de l’étude AHA 2013 – D’après Giugliano R et al., LBCT.05-04, actualisé FA documentée par ECG dans les 12 derniers mois CHADS2 ≥ 2 (n = 21 105) Randomisation1:1:1 randomisation stratifiée en fonction CHADS2 score 2-3 versus 4-6et de la nécessité de réduction de dose d’edoxaban * Double-aveugle, Double-placebo Warfarine(INR 2,0-3,0) Edoxaban forte dose60* mg x 1/j Edoxaban faible dose30* mg x 1/j *Dose diminuée de 50 % si : - CrCI 30-50 ml/mn - poids ≤ 60 kg - inh. puissant P-gp Critère principal d’efficacité = AVC ou ETE Critère IIaire efficacité = AVC ou ETE ou mortalité CV Critère principal tolérance = saignements majeurs (ISTH) Non-infériorité lim sup 97,5 % CI < 1,38 ISTH : international society on thrombosis and haemostasis ;P-gp : P-glycoproteine ; ETE : évthrombo-embolique.
ENGAGE-TIMI 38 : edoxaban versus warfarine(2) Critère principal : AVC/ETE (médiane de 2,8 années de suivi) AHA 2013 – D’après Giugliano R et al., LBCT.05-04, actualisé p non-infériorité p supériorité Analyse non infériorité (ITTm, OT) HR (IC97,5) 0,79 Edoxaban 60* mg x 1/j vs warfarin p < 0,0001 p = 0,017 1,07 Edoxaban 30* mg x 1/j vs warfarin p = 0,005 p = 0,44 1,38 0,50 1,00 2,0 Edoxaban non inférieur p supériorité Analyse supériorité (ITT, tous) HR (IC97,5) 0,87 Edoxaban 60* mg x 1/j vs warfarin p = 0,08 1,13 Edoxaban 30* mg x 1/j vs warfarin p = 0,10 0,50 1,00 2,0 Edoxaban supérieur Edoxaban inférieur
ENGAGE-TIMI 38 : edoxaban versus warfarine(3) Critères secondaires principaux AHA 2013 – D’après Giugliano R et al., LBCT.05-04, actualisé Edoxaban 60* mg x 1/j vs warfarin Edoxaban 30* mg x 1/j vs warfarin Warfarine TTR 68,4 % p vs warfarine HR (IC95) 0,54 0,33 AVC hémorragique < 0,001 < 0,001 1,00 1,41 0,97 < 0,001 AIT 0,87 0,005 0,32 2e : AVC, ETE, décès CV 0,95 0,87 Décès ou hém.intra-cranienne 0,004 < 0,001 0,82 0,92 Mortalité toutes causes 0,08 0,006 0,87 0,86 0,013 0,008 Décès CV 0,85 0,94 IDM 0,60 0,13 1,19 *Dose réduite de 50 %chez patients sélectionnés 0,25 0,5 1,00 2,0 Edoxaban supérieur Edoxaban inférieur
ENGAGE-TIMI 38 : edoxaban versus warfarine(4) Conclusions AHA 2013 – D’après Giugliano R et al., LBCT.05-04, actualisé Diminution de 14-15 % de la mortalité CV • En comparaison à un traitement par warfarine bien contrôlé (TTR 68,4 %), l’edoxaban 30 ou 60 mg/j en une prise par jour est : • Non inférieur pour AVC/événements emboliques systémiques - ETE (2 dosages) • Le dosage à 60 mg diminue AVC/ETE sous Tt • Les 2 dosages (60/30 mg) diminuent significativement : • Les saignements majeurs (20/53 %) • Les AVC hémorragiques (46/67 %) • Les décès CV (14/15 %) • Les hémorragies intra-crâniennes (53/70 %)