Download
1 / 20
250 likes | 661 Views
Spina Bifida: An Overview. Sarah Winter, MD. Spina Bifida tutorial objectives. Exposure to some helpful terminology Describe the anatomy of spina bifida Describe common treatments of spina bifida Describe the Spina Bifida Clinic. Terminology.

E N D
Spina Bifida: An Overview Sarah Winter, MD
Spina Bifida tutorial objectives • Exposure to some helpful terminology • Describe the anatomy of spina bifida • Describe common treatments of spina bifida • Describe the Spina Bifida Clinic
Terminology • Spina Bifida: the commonly used term for the defect of the spine and vertebral bodies which did not fuse in utero • Spina Bifida Occulta: this term refers only to a defect in the boney elements of the vertebral column. This is not the same as spina bifida as these people do not typically experience any problems related to the defect.
Terminology • Myelomeningocele: This is a more anatomically correct term for spina bifida but most lay people do not use it. It is Latin for “ there is a sack (cele) containing the meninges and spinal cord (myelo)”. • Meningomyelocele: This is the same thing • Myelodysplasia: This is also the same thing but it is confusing because this is also the name of a cancer of the blood. So, this term is not recommended. • Encephalocele: This is when the brain itself protrudes from the skull in a sack (cele). This is not usually compatible with life.
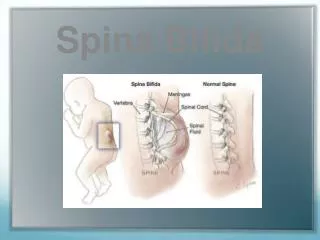
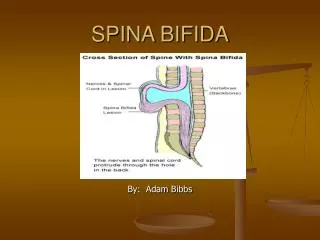
Anatomy Spina bifida occurs when the neural tube (pictured here) fails to close. The severity of the child’s problems depends on where the tube failed to close. The higher the level of the opening, the more severe the problems. This all happens by day 28 of pregnancy when most often, a women is not yet aware that she is pregnant. This is why it is recommended to take folic acid supplements which are known to prevent neural tube defects, before becoming pregnant.
Anatomy The drawings to the right are a representation of the different ways spina bifida can appear.
Anatomy This is a large lesion in the middle of the back This is a small lesion in the lower end of the spine
Anatomy This is what it looks like after the repair is done. The neurosurgeon can repair the skin and fix the sack. But the nerve damage cannot be repaired.
Anatomy In addition to the spinal cord defect, most children with spina bifida have a Chiari, Type II malformation. This is a brain malformation that is illustrated in the picture on the top right, The fluid filled spaces of the brain can get too big (hydrocephalus) because the brainstem can be malformed and too far down into the neck area blocking the easy flow of cerebral spinal fluid. Some children need a shunt placed to drain the extra fluid out. The shunt goes from the ventricle to the belly. It is easy to see a shunt in a baby but older children and adults’ head size and hair make it difficult to see. The Chiari malformation may also contribute to the learning difficulties many of these children have.
Anatomy Problems from nerves that don’t work: When the nerves aren’t formed right, lots of problems can happen. Mobility problems because the nerves to the legs are affected either completely or partially Bladder function problems: this almost always happens as the bladder nerves are very low in the spinal cord Bowel function problems; again this is very frequent as nerves to the lower intestine and rectum are low in the spinal cord Sensation: below the level of the lesion there may be areas that have no sensation. This can cause skin problems.
Treatment options Initial repair: The initial repair is usually done within the first day of life. Babies born with spina bifida benefit by having a prenatal diagnosis so the mother can deliver at a hospital that has a pediatric neurosurgeon who can do the repair and the baby does not have to be transferred. In utero surgery has been done for approximately 15 years. This is when the repair is done through a small incision in the mother’s womb at about 28 weeks of gestation. It is not yet clear if the outcome is better although less of these babies need a shunt.
Treatment: Shunt placement for hydrocephalus Shunt: In about 60 -70% of children with spina bifida, a shunt is required to prevent enlargement of the head due to increased cerebral spinal fluid in the ventricles. Most shunts are placed so that the fluid drains from the ventricle into the peritoneal or abdomen (VP shunt). Sometimes the shunt is placed so that the fluid drains from the ventricle to the atrium of the heart (VA shunt)
Treatment: Bladder cath for neurogenic bladder Because the nerves to the bladder are often not functioning well in people with spina bifida, the bladder becomes very distended from not passing urine. Therefore, every 4 hours while awake, most people with spina bifida insert a catheter into the bladder to allow urine to pass. This prevents many complications of the kidneys. Before this treatment was available, many people with spina bifida had kidney failure.
Treatment: orthopedic deformities Club feet are common in babies with spina bifida. The nerves leading to the feet are often damaged and so the feet form abnormally in utero. This can be corrected with casts and/or surgery right after the baby is born.
Treatment: orthopedic deformities Scoliosis is another common orthopedic problem. As the vertebral bodies around the defect are usual malformed, it makes sense that the spine may not grow straight. This photo shows an extreme situation. The complication rate for repair of these deformities is higher than other types of scoliosis because the skin and blood vessels around the deformity are not normal with good blood flow to healthy tissue. Therefore, these patients should be operated on by highly experienced spine surgeons in complex spinal deformities in children.
Treatment: mobility problems Children with spina bifida often lack the muscle strength and sensation to walk without assistive devices. Fortunately, technology allows better and better bracing for improved mobility. As children grow and gain weight, it becomes harder to move around with heavy and cumbersome bracing. Mobility, not walking should be the goal. This child will likely choose to use a chair for most of her activities as she gets older because it is faster and allows her to participate more typically in her life.
Treatment: mobility problems This young man is highly competitive in his adaptive wheelchair made specifically for his sport. He has another chair for his daily activities.
Treatment: skin problems Skin sores are common in children with spina bifida. The best treatment for skin issues is prevention. Skin inspection daily is critical. Awareness that heat, cold, abrasions, and lacerations will not be perceived by the child with spina bifida may help families avoid those damaging situations. This takes constant vigilance. Even the most careful patient and family may experience skin damage. This foot sore pictured is caused by pressure on the foot. The plan outlined is an example of some of the treatment options to prevent worsening of a sore.
Spina Bifida Clinic • Spina Bifida Clinic is a multidisciplinary clinic involving the following disciplines: • Orthopedics • Neurosurgery • Urology • Nursing • Neurology • OT • PT • Genetics
Spina Bifida Clinic • Three Friday mornings a month • Director of the Clinic: Paula Peterson, PNP (previous URLEND faculty member) • Follows approximately 350 children with neural tube defects • Participates in a national registry