Download
1 / 32

E N D
Streptococci assist. Prof. Zainab Abdul jabarAldhaher
Streptococcus is a genus of sphericalGram-positivebacteria belonging to the phylumFirmicutes] and the lactic acid bacteria group. Cellular division occurs along a single axis in these bacteria, and thus they grow in chains or pairs, hence the name. Contrast this with staphylococci, which divide along multiple axes and generate grape-like clusters of cells.
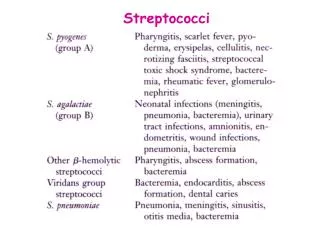
Streptococci comprise a diverse group of Gram-positive cocci, which continuously undergo taxonomic revision. They are distributed widely in humans and animals, mostly forming part of their normal flora. A few species cause significant human morbidity. The oral streptococci, which include the cariogenic mutansgroup, are important members of the genus. Streptococci General properties Characteristics They are catalase-negative, Gram-positive spherical or oval cocci in pairs and chains; 0.7–0.9 μm in diameter. Chain formation is best seen in liquid cultures or pus.
Streptococci • Characters of Streptococci • Gram positive cocci • Chains or pairs • Usually capsulated • Non motile • Non spore forming • Facultative anaerobes • Fastidious • Catalase negative (Staphylococci are catalase positive)
Classification of Streptococci • Streptococci can be classified according to: • Oxygen requirements • Anaerobic (Peptostreptococcus) • Aerobic or facultative anaerobic (Streptococcus) • Serology (Lanciefield Classification) • Hemolysis on Blood Agar (BA)
Optochin Susceptibility Test • Principle: • Optochin (OP) test is presumptive test that is used to identify S. pneumoniae • S. pneumoniae is inhibited by Optochin reagent (<5 µg/ml) giving a inhibition zone ≥14 mm in diameter. • Procedure: • BAP inoculated with organism to be tested • OP disk is placed on the center of inoculated BAP • After incubation at 37oC for 18 hrs, accurately measure the diameter of the inhibition zone by the ruler • ≥14 mm zone of inhibition around the disk is considered as positive and ≤13 mm is considered negative • S. pneumoniae is positive (S) while S. viridans is negative (R)
Serology: Lanciefield Classification • Streptococci classified into many groups from A-K & H-V • One or more species per group • Classification based on C- carbohydrate antigen of cell wall • Groupable streptococci • A, B and D (more frequent) • C, G and F (Less frequent) • Non-groupable streptococci • S. pneumoniae (pneumonia) • viridans streptococci • e.g. S. mutans • Causing dental carries
group A includes the important human pathogen Streptococcus pyogenes • group B contains one species, Streptococcus agalactiae, an inhabitant of the female genital tract; it causes infection in neonates • group C mainly causes diseases in animals • group D includes the enterococci (Enterococcus faecalis, etc.) and ranks next to group A in causing human disease.
Classification of Streptococci Based on Hemolysis on Blood Agar • Hemolysis on BA • -hemolysis • Partial hemolysis • Green discoloration around the colonies • e.g. non-groupable streptococci (S. pneumoniae & S. viridans) • -hemolysis • Complete hemolysis • Clear zone of hemolysis around the colonies • e.g.Group A & B (S. pyogenes & S. agalactiae) • -hemolysis • No lysis • e.g. Group D (Enterococcus spp)
Hemolysis on Blood agar -hemolysis -hemolysis -hemolysis
Transmission • Most streptococci are part of the normal flora of the human throat, skin, and intestines but produce disease when they gain access to tissues or blood. Viridans streptococci and S. pneumoniae are found chiefly in the oropharynx;S. pyogenes is found on the skin and in the oropharynx in small numbers; S. agalactiae occurs in the vagina and colon; and both the enterococci and anaerobic streptococci are located in the colon.
Group A streptococci • Include only S. pyogenes • Group A streptococcal infections affect all ages peak incidence at 5-15 years of age • 90% of cases of pharyngitis
Pathogenesis and Virulence Factors • Structural components • M protein M, which interferes with opsonization and lysis of the bacteria • Lipoteichoic acid & F protein adhesion • Hyaluronic acid capsule, which acts to camouflage the bacteria • Enzymes • Streptokinases • Deoxynucleases • C5a peptidase • Pyrogenic toxins that stimulate macrophages and helper T cells to release cytokines • Streptolysins • Streptolysin O lyse red blood cells, white blood cells, and platelets • Streptolysin S facilitate the spread of streptococci through tissues
Disease caused by S. pyogenes • Suppurative • Non-Invasive • Pharyngitis (“strep throat”)-inflammation of the pharynx • Skin infection, Impetigo • Invasive • Scarlet fever-rash that begins on the chest and spreads across the body • Pyoderma-confined, pus-producing lesion that usually occurs on the face, arms, or legs • Necrotizing fasciitis-toxin production destroys tissues and eventually muscle and fat tissue • Non Suppurative • Rheumatic fever: Life threatening inflammatory disease that leads to damage of heart valves muscle • Glomerulonephritits • Immune complex disease of kidney • inflammation of the glomeruli and nephrons which obstruct blood flow through the kidneys
Differentiation between -hemolytic streptococci • The following tests can be used to differentiate between -hemolytic streptococci • Lanciefield Classification • Bacitracin susceptibility Test • Specific for S. pyogenes (Group A) • CAMP test • Specific for S. agalactiae (Group B)
Bacitracin sensitivity • Principle: • Bacitracin test is used for presumptive identification of group A • To distinguish between S. pyogenes (susceptible to B) & non group A such as S. agalactiae (Resistant to B) • Bacitracin will inhibit the growth of gp A Strep. pyogenes giving zone of inhibition around the disk • Procedure: • Inoculate BAP with heavy suspension of tested organism • Bacitracin disk (0.04 U) is applied to inoculated BAP • After incubation, any zone of inhibition around the disk is considered as susceptible
CAMP test • Principle: • Group B streptococci produce extracellular protein (CAMP factor) • CAMP act synergistically with staph. -lysin to cause lysis of RBCs • Procedure: • Single streak of Streptococcus to be tested and a Staph. aureus are made perpendicular to each other • 3-5 mm distance was left between two streaks • After incubation, a positive result appear as an arrowhead shaped zone of complete hemolysis • S. agalactiae is CAMP test positive while non gp B streptococci are negative
Differentiation between -hemolytic streptococci • The following definitive tests used to differentiate between S. pneumoniae & viridans streptococci • Optochin Test • Bile Solubility Test • Inulin Fermentation
Optochin Susceptibility Test Optochin resistant S. viridans Optochin susceptible S. pneumoniae
Bile Solubility test • Principle: • S. pneumoniaeproduce a self-lysing enzyme to inhibit the growth • The presence of bile salt accelerate this process • Procedure: • Add ten parts (10 ml) of the broth culture of the organism to be tested to one part (1 ml) of 2% Na deoxycholate (bile) into the test tube • Negative control is made by adding saline instead of bile to the culture • Incubate at 37oC for 15 min • Record the result after 15 min
Bile Solubility test • Results: • Positive test appears as clearing in the presence of bile while negative test appears as turbid • S. pneumoniae soluble in bile whereas S. viridans insoluble
Differentiation between -hemolytic streptococci Differentiation between -hemolytic streptococci
STREPTOCOCCUS PNEUMONIAE • Diseases • Pneumococci cause pneumonia, bacteremia, meningitis, and infections of the upper respiratory tract such as otitis media and sinusitis. Pneumococci are gram-positive lancet-shaped cocci arranged in pairs (diplococci) or short chains. (The term “lancet-shaped” means that the diplococci are oval with somewhat pointed ends rather than being round.) On blood agar they produce alpha-hemolysis. In contrast to viridans streptococci, they are lysed by bile or deoxycholate and their growth is inhibited by optochin.
Pneumococci possess polysaccharide capsules of more than 85 antigenically distinct types. With type-specific antiserum, capsules swell (quellung reaction), and this can be used to identify the type. Capsules are virulence factors; i.e., they interfere with phagocytosis and favor invasiveness. Specific antibody to the capsule opsonizes the organism, facilitates phagocytosis, and promotes resistance. Such antibody develops in humans as a result either of infection (asymptomatic or clinical) or of administration of polysaccharide vaccine. Capsular polysaccharide elicits primarily a B-cell ( i.e., T-independent) response.
Another important surface component of S. pneumoniae is a carbohydrate in the cell wall called C-substance. This carbohydrate is medically important, not for itself, but because it reacts with a normal serum protein made by the liver called C-reactive protein (CRP). CRP is an “acute-phase” protein that is elevated as much as a 1000-fold in acute inflammation. CRP appears to be a better predictor of heart attack risk than an elevated cholesterol level.
Pneumococci are a prominent cause of otitis media, sinusitis, purulent bronchitis, pericarditis, bacterial meningitis, and sepsis, especially in immunocompromised patients. • Treatment • Most pneumococci are susceptible to penicillins and erythromycin. In severe pneumococcal infections, penicillin G is the drug of choice, whereas in mild pneumococcal infections, oral penicillin V can be used. In penicillin-allergic patients, erythromycin or one of its long-acting derivatives, e.g., azithromycin
Oral streptococci Streptococci have been isolated from all sites in the mouth and comprise a large proportion of the resident cultivable oral microbiota. Oral streptococci are generally alpha-haemolytic (partial haemolysis) on blood agar, and early workers called them viridans streptococci. Oral streptococci can be divided into four main species groups as follows: 1. mutansgroup 2. salivariusgroup 3. anginosusgroup 4. mitisgroup. Each of these groups comprises a number of species.
Mutans group (mutans streptococci) potential role in the aetiology of dental caries. Streptococcus mutanswas originally isolated from carious human teeth by Clarke in 1924 and shortly afterwards, was recovered from a case of infective endocarditis. Mutans streptococci are recovered almost exclusively from hard, non-shedding surfaces in the mouth, such as teeth or dentures, Mutans streptococci are regularly isolated from dental plaque at carious sites and can act as opportunistic pathogens, being isolated from cases of infective endocarditis. is generally a result of their entry into the blood stream during intraoral surgical procedures (e.g. tooth extraction) , Treatment and prevention In patients at risk of infective endocarditis (e.g. those with damaged or prosthetic heart valves), prophylactic antibiotic cover should always be given before dental procedures.
Gelatinous colonies of mutansstreptococci mainly comprising extracellular polysaccharides