Download
1 / 36
380 likes | 749 Views
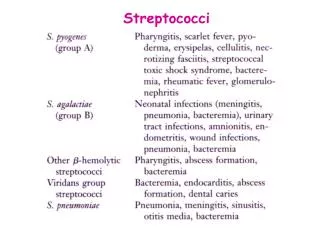
Streptococci and Enterococci. Gregory Raines, PA-C Franklin Pierce PA Program. Streptococci. Streptococci are Gram-positive cocci that grow in chains or pairs. Cell division occurs in a single plane resulting in chains. Streptococci are unable to synthesize heme.

E N D
Streptococci and Enterococci Gregory Raines, PA-C Franklin Pierce PA Program
Streptococci • Streptococci are Gram-positive cocci that grow in chains or pairs. • Cell division occurs in a single plane resulting in chains. • Streptococci are unable to synthesize heme. • Streptococci are catalase negative. The catalase test is the common test used to distinguish Streptococcus species from Staphylococcus species. Streptococci lacks the enzyme catalase which catalyzes the reaction H2O2 O2 + H2O. • Streptococci are auxotrophic, and need to be cultured on enriched media to grow. Usually sheep blood agar plates are used. • Streptococci are typically grouped by hemolysis on blood agar plates: Alpha hemolysis occurs when the RBCs are intact, but hemoglobin is converted to biliverdin. This causes a greening of the plate. Beta hemolysis is true hemolysis due to the actions of a hemolysin, an erythrocyte lysing enzyme. The plate becomes clear where the blood cells have been lysed. (When in doubt, see if you can read your lab book through the zone of hemolysis. If you can read the text, you have beta-hemolysis!) Gamma hemolysis is a misnomer, there is actually no hemolysis.
Alpha hemolysis Beta hemolysis Gamma hemolysis Enterococcus faecalis Streptococcus pneumoniae
Alpha hemolytic streptococci are classified by the results of their culture in the presence of optochin or their solubility in bile. Viridans Streptococcus Streptococcus pneumoniae
Streptococcus pneumoniae • Commonly called the pneumococcus, used to be called Diplococcus pneumoniae - was isolated in 1881 by Pasteur and later shown to be the major cause of lobar pneumonia (infecting one or more lobes of the lung) in humans. • On Gram stain, S. pneumoniae appears as Gram-positive, lancet-shaped diplococci. Habitat: normal commensal of the upper respiratory tract. Pathogenicity appears to result primarily from capsule. If strain loses capsule it is readily phagocytosed. Immunity is directed against capsule and is therefore type specific.
Virulence Factors of Streptococcus pneumoniae * The capsule is the most important virulence factor.It is composed of repeating oligosaccharide units. 84 types (potentially >100 types) exist, and immunity is type specific. 23 types cause most of the infections. The capsule interferes with the opsonizing activity of the alternative complement pathway. Antibody against the capsule is needed because C3b only binds to the cell wall and hence is buried by the capsule. There is a vaccine of the 23 polysaccharide antigens. It should be given to the elderly or to those with underlying conditions, like lung disease, that predispose them to disease from S. pneumoniae. Now there is a vaccine for children that conjugates the capsular polysaccharides of the 7 most common invasive pneumococci to a protein. • Inflammation is stimulated by the release of teichoic acid and PDG during autolysis. It is not caused by the capsule. Releasedteichoic acid stimulates production of platelet activating factor (PAF), and mimics PAF activity. Peptidoglycan binds to Toll-like receptor 2 on macrophages and induces the secretion of cytokines. The combination probably explains the pathology (the influx of fluid into the alveoli, followed by red cells and then neutrophils) observed in pneumococcal pneumonia. • Pneumolysin is a cytolysin that forms pores when inserted into eukaryotic membranes. In vitro studies have lead to lots of conjecture about what pathology it causes. The most current explanation is that since in vitro studies show that it is cytotoxic to bronchial epithelial cells, it may screw up the clearance mechanism, allowing the bacteria to remain in the lower respiratory tract and grow. Also, it could attack macrophages and neutrophils as well as make the alveolar-capillary barrier leak. • Neuraminidase may unmask cell-surface binding receptors and its effect on the red cell membrane may contribute to the unusual complication of hemolytic-uremic syndrome (HUS) in some patients with severe pneumococcal infection. • Hyaluronidase may facilitate tissue spread. • IgA1 proteases may prevent IgA-mediated immune clearance. • How it sticks to host cells and what it adheres to is not understood.
Pneumococcal Pneumonia • Accounts for about one million deaths per annum worldwide. • Has a 10 - 20% mortality but in the over-70 years age group, mortality is as high as 70%. Incidence varies enormously according to age (highest in aged) occupation, living conditions. In closed groups, incidence is 10 - 20 x higher. • South African Gold miners have 100x the rate in the general population. • Acute lung inflamation - lobar - involving the tissues of the lung. • Begins abruptly with shaking chills, fever and pleural pain. Cough with production of sputum - pink to rusty in color. Alvioli fill with exudate. Bacteremia occurs in 25%. • Pneumococci may invade other tissues, eg.sinuses, middle ear and meninges. • Recovery is abrupt and coincides with appearance of circulating antibodies. [Note: many other causes of pneumonia - Mycoplasma pneumoniae, Legionella, etc.] Pneumococcal Meningitis • With Neisseria meningitidis and Haemophilus influenzae, Pneumococcus is one of the three leading causes of bacterial meningitis. • Bacteremia occurs in >80%. • Sinusitis and Otitis Media • Also cause of middle ear infection - frequently occurs in children in association with viral infection • Common cause of sinusitis
Chest X-ray reveals: multilobar involvement: RML, superior segment RLL, and LLL infiltrates
Treatment • Used to be uniformly penicillin (PCN) sensitive. However, resistance to b-lactams are emerging and spreading via transformation. (This means that you must test sensitivities of the various antibiotics on the specific pathogen that was isolated from a patient.) • Alternative effective agents include the cephalosporins, fluoroquinolones, erythromyicn. • Vaccine has been made containing polysaccharide from 23 of the most prevalent types. Gives 75 - 95% protection. Recommended for high-risk groups, eg. those with chronic diseases, elderly, etc.
Growth on Optochin = The Viridans Streptococci • The viridans streptococci are normal flora - they colonize the oropharynx, Gastrointestinal and genitourinary tracts. • At least 24 species have been identified and they are classified into 5 different subgroups: S. anginosus S. bovis S. mitis S. mutans S. salivarius • Although these organisms can cause a variety of diseases, they are most commonly associated with dental carries, subacute bacterial endocarditis, and suppurative intra-abdominal infections.
b-Hemolytic Streptococci: An Overview • The b-hemolytic streptococci are further divided into groups based on their Lancefield antigen. This is a cell wall carbohydrate that is characteristic of that particular Group of b-hemolytic streptococci. The only exception is the former Group D streptococci (now a separate genus: Enterococcus) that have glycerol teichoic acid as their Lancefield antigen. • Lancefield's serogroup classification - A - O - based on C carbohydrate antigen, extracted from cells by heating at 150oC. Group A are primary human pathogens - S. pyogenes Group B - cattle and humans Group D - intestinal tract of man and animals (enterococci) E. faecalis Group E - swine etc.
Group A Streptococcus pyogenes • Among the beta-hemolytic streptococci, Streptococcus pyogenes is the most virulent for humans. • Streptococcus pyogenes is spread person to person by respiratory secretions. Can survive on dry surfaces for long periods of time. • Asymtomatic colonization in the upper respiratory tract and skin are common (15-20%) - usually only transient. • Diseases caused by Streptococcus pyogenes: Throat and Respiratory Tract: Strep Throat,cervical lymphadenitis, peritonsillar abscess, pneumonia Skin: Impetigo, Cellulitis, Erysipelas, Necrotizing Fasciitis Post Streptococcal sequelae: Rheumatic fever, which can follows pharyngitis due to S. pyogenes; Glomerulonephritis, which can follow either pharyngitis or impetigo. Toxin Mediated Disease: Scarlet Fever, Streptococcal Toxic Shock Syndrome • Streptococcus pyogenes is sensitive to bacitracin (99%).This is the basis of a diagnostic test because all other b-hemolytic streptococci are resistant (95%).
A. Surface Constituents M protein • M protein is required for virulence- 80+ types! It looks like a human protein since it has a coiled-coil a-helical structure • M protein extends from cell envelope as fimbriae. Its carboxy terminal is attached to PDG and shows little variability. Its negatively charged amino terminal is outside the cell and is variable. • Certain M protein types areassociated with pharyngitis or with skin infections. Likewise, specific M protein types are associated with the rheumatic fever and glomerulonephritis. Shared epitopes between M protein and host tissues may contribute to the pathogenesis of rheumatic fever and complicate the design of an M protein-based vaccine for Streptococcus pyogenes. • M protein prevents phagocytosis by preventing complement opsonization. It has a site that binds factor H which in turn binds C3b leading to the hydrolysis of C3b to its inactive form by Factor I. • M protein adheres to epithelial cells. • M protein binds fibrinogen that can then bind plasminogen. The streptokinase of Streptococcus pyogenes can then convert it to bound plasmin facilitating the organisms spread through tissues. • Antibody to a specific N terminus provides immunity to that M type, but not to others. Thus one can be infected with Streptococcus pyogenes repeatedly in one’s life. Lipoteichoic acid (LTA) • LTA is attached to M protein. • It may allow binding to fibronectin.
F protein • F protein allows binding to fibronectin. • F protein may or may not bind respiratory epithelial cells. F protein mutants will not bind Langerhans cells but will bind keratinocytes Hyaluronic acid capsule • The capsule inhibits phagocytosis. C5a protease: • C5a protease cleaves the C5a component of complement and inhibits neutrophil chemotaxis in vitro. The role in pathogenesis unknown. IgG and IgA binding proteins: • These proteins bind the Fc region of IgG or IgA. Group A carbohydrate • The Group A carbohydrate is also known as the Group A Lancefield antigen. • It stimulates antibody production, but the antibodies produced are not opsonic. • It has an unknown role in pathogenesis, but this is the molecule that the rapid strep test uses to identify Group A strep infections.
B. Secreted Virulence Factors Hyaluronidase • Hyaluronidase destroys hyaluronic acid. This could be important in the spread through tissue during cellulitis. Streptolysin O • This oxygen labile (inhibited by oxygen) hemolysin that is only active in its reduced form. It causes beta hemolysis, and is produced by most Group A strains • Streptolysin O works by inserting directly into the host cell membrane forming transmembrane pores. • It is antigenic, and can be used to test for evidence of recent streptococcal infection. Streptolysin S • Streptolysin S is oxygen stable, and made in the presence of serum. • It is a hemolysin causing the beta-hemolysis seen on blood agar plates. • It is structurally similar to a bacteriocin. • Streptolysin S is nonantigenic. • Streptolysin S is one of the most potent cytotoxins known and is capable of a wide variety of host cells. • Streptolysin S is a virulence factor in the pathogenesis of invasive infections such as necrotizing fasciitis.
Streptokinase • Streptokinase hydrolyzes fibrin and other host proteins helping the organism spread through tissues. • The purified enzyme is used clinically to dissolve blood clots. • Streptokinase is antigenic, and antibody against it can neutralize its enzymatic activity. Only used once Cysteine Protease • Degrades a large array of proteins, both in host tissues and those expressed on the bacteria’s own surface. Streptococcal Pyrogenic Exotoxins and Related Superantigens • Various strains of Streptococcus pyogenes can produce a large number of potential superantigens. • The best recognized are the streptococcal pyrogenic exotoxins (SPE-A, SPE-C, SPE-F, etc.) • SPE-A and SPE-C are encoded on lysogenic phage • SPE-A is the cause of scarlet feverand is implicated as a key factor many cases of streptococcal toxic shock syndrome complicating invasive infections such as necrotizing fasciitis.
Streptococcal pharynigitis • most frequent Strep A infection - sore throat. May lead to tonsilitis. • Develops 2-4 days after exposure to the pathogen - abrupt onset of sore throat, fever, malaise, headache. • Posterior pharynx - erythematous with exudate and cervical lymphadenopathy. • Antibiotic tx initiated within 10 days from onset of symptoms can prevent rheumatic fever.
Scarlet fever • Usually result of Strep sore throat caused by a pyrogenic toxin-producing organism - toxin encode by phage. • Fever, diffuse erythematous rash. • A yellowish white coating initially covers the tongue which is later shed revealing a red, raw surface underneath (“strawberry tongue”) • Rash disappears over 5-7 days and is followed by desquamation. • Three antigenically distinct toxins (A, B and C) - immunity to one does not protect against the others.
Streptococcal impitigo (Pyoderma) • Impetigo is a superficial vesiculopustular skin infection occurring prominently on exposed areas of the face and extremities. Affected patients usually have multiple lesions but little or no systemic toxicity. • The infection usually occurs in warm, humid conditions. Poverty, crowding, and poor personal hygiene promote impetigo which is easily spread within families. Infection typically arises at the site of minor skin trauma such as insect bites or abrasions. Carriage of group A streptococcus (GAS) and S. aureus predisposes to subsequent impetigo • Staphylococcus aureus is also commonly present in the lesion
Erysipelas • Acute infection of the skin - local pain and inflammation, lymph node enlargment and systemic signs. • Erysipelas is a characteristic form of cellulitis which affects the superficial epidermis, producing marked swelling. The resulting local changes are unique to erysipelas and are not seen in other forms of cellulitis. • Most common in children or older adults • Historically on the face Cellulitis • Unlike erysipelas involves skin and deeper subcutaneous tissue. • Indentification of the organism is necessary since many different microbes can cause cellulitis.
Necrotizing fasciitis • Infection that occurs deep in the subcutaneous tissue, spreads along the fascial planes and is characterized by rapid destruction of muscle and fat. • Initially there is evidence of cellulitis, after which bullae form and gangarene and systemic symptoms. • Mortality exceeds 50% • Need both antibiotic tx as well as surgical debridement.
Nonsuppurative infections • organism is not present in the affected organ. • Rheumatic fever: It occurs in a small percentage of individuals, 2 - 3 weeks after an untreated pharyngeal infection that was caused by a b hemolytic group A Strep. Recovery occurs without residual injury to the joints but serious damage to heart valves cause rheumatic heart disease. • used to be one of the most common heart conditions but due to the great decrease in the incidence of rheumatic fever it is now rare in younger people. However, still a major problem in developing countries and in overcrowded conditions – leading cause of heart disease in developing countries. • May be an immunological reaction - antibody to Strep also binding to heart tissue. • Patients with a history of rheumatic fever require long-term antibiotic prophylaxis to prevent recurrence of the disease. Because damage to the heart valves predisposes them to endocarditis - antibiotic prophylaxis is also required prior to procedures that can produce a transient bacteremia (eg. dental procedures) • Glomerulonephritis: Most cases of glomerulonephritis occur about a week after group A Strep infection (skin or throat). Also thought to be an immunolgical reaction in which a Strep directed antibody reacts with the glomerular basement membrane; or antibody-antigen complexes are deposited onto basement membrane. Leads to loss of protein (blood initially in urine) through kidneys and hypertension. Can lead to chronic glomerulonephritis and kidney failure in adults (young patient generally have an uneventful recovery).
Treatment • S. pyogenes is very sensitive to penicillin. • Cephalosporin or Erythromycin (5% resistance) are also effective tx. • In mixed infections may need to broaden coverage to cover S. aureus (oxacillin or vancomycin) • Drainage and surgical debridment are needed in serious soft tissue infections • In serious Group A strep infections combination of PCN and clindamycin should be given. (Clindamycin suppresses exotoxin and M-protein production)
ß-Hemolytic StreptococcusGroup B (Streptococcus agalactiae) Epidemiology of ß-Hemolytic Streptococcus Group B • Group B streptococci (GBS) are split into typesbased on the surface polysaccharide capsular antigens [I (Ia, Ib/c, Ia/c), II, III, IV, V and VI). • GBS is part of the normal vaginal and/or intestinal flora in 20-30% of adults. • Children are more susceptible to GBS infection than adults. • In babies, the infection can be acquired when the organism, which has colonized the vagina, ascends and infects the amniotic fluid through the placental membranes. The fetus then aspirates the organism in the infected amniotic fluid. Alternatively, infection can be acquired during the passage through the birth canal.
Diseases causes by GBS • GBS is the leading cause of pneumonia, septicemia and meningitis in newborns. (2-3 cases /1000 births) • GBS can easily be detected by doing a rectal + vaginal culture around the 37th week of pregnancy. A colonized mother can then be treated with antibiotics when she enters labor to reduce transmission. Early Onset Infections: Pneumonia and Septicemia • These infection occur in first days of life • Risk factors include premies with low birth weight, and premature rupture of the membranes. • Presents like respiratory distress syndrome (RDS). Fever is present. • On autopsy, widespread injury to lung tissue with alveolar hemorrhage and protein exudate. • All capsule types are implicated. Late Onset Infections: Bacteremia and Meningitis • GBS is the most common agent of meningitis in 5-30 day olds. (Although it can be seen as late as 6 months). • Capsule type III is themost prevalent (70-80%). • GBS strains have the ability to cross the blood-brain barrier though attachment and invasion of the brain capillary cells. • Foot ulcers in diabetics • Bovine mastitis in cows. GBS is also a very important bovine pathogen.
Enterococcus (previously known as b-Hemolytic StreptococcusGroup D) Identification and Epidemiology • The enterococci are normal flora of the intestinal tract. • Common species to recognize include Enterococcus faecalis and Enterococcus faecium. • The enterococci cause disease when they find themselves out of their normal places. The most common diseases due to the enterococci are: • Urinary Tract Infections, especially in older men with prostate problems. • Endocarditis if in blood • Frequently, it is one of the genera found in abscesses that originate from intestinal flora. • The enterococci can metabolize esculin to a black pigment and grow in 40% bile and high salt (6.5%). Streptococcus bovis can also grow in bile and metabolize esculin, but it cannot grow in high salt. Treatment • Penicillin or ampicillin remain the drug of choice for tx of enterococcal infections such as urinary tract infections, peritonitis, and wound infections that do not require bactericidal treatment. Vancomycin is an alternative for PCN allergic patients or for organisms that are PCN resistant. • Therapy traditionally consists of an aminoglycoside and a cell wall-active antibiotic (ampicillin or vancomycin) for the tx of enterococcal endocarditis or meningitis. • Resistance to aminoglycosides, PCN and vancomycin has become a major problem. • >25% resistance to aminoglycosides • >50% of some species resistant to ampicillin (eg. E. faecium) • >20% vancomycin resistance (VRE) • Resistance to aminoglycosides and vancomycin is mediated by plasmids and can be potentially transferred to other bacteria. • Newer agents such as Linezolid, Quinupristin/Dalfopristin, Daptomyocin can be used to tx resistant organisms.
References 1. Medical Microbiology 4th Edition. Murray PR, Rosenthal KS, Kobayashi GS, Pfaller MA. 2. USCD www.ratsteachmicro.com 3. Principles and Practice of Infectious Diseases. Mandell, Douglas, and Bennett