Download

1 / 55
550 likes | 561 Views
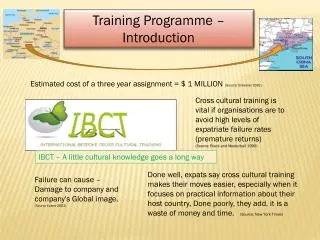
HE EoE ACCS Training Programme. An Overview Chris Maimaris. Objectives. Outline of ACCS Structure and supervision WPBAs Annual Appraisals-ARCP Revalidation Who to ask for advice Regional Days. CCT Pathway, 2015 curriculum. CCT in EM +/- sub-specialty.

E N D
HE EoE ACCS Training Programme An Overview Chris Maimaris
Objectives • Outline of ACCS • Structure and supervision • WPBAs • Annual Appraisals-ARCP • Revalidation • Who to ask for advice • Regional Days
CCT Pathway, 2015 curriculum CCT in EM +/- sub-specialty CCT Anaesthesia +/- sub-specialty CCT in AM or specialisms FCEM Exit Exam FRCA Exam ST4, ST5, ST6 in EM Traditional SpR posts ST3, ST4, ST5 ST6 ST7 MG posts ST3, ST4, ST5, ST6 AM and speciallties MRCP +Paces MCEM Part B&C FRCA Part I CT3 12 months EM Paediatric EM CT2 12 months Anaesthetics CT3 12 months Medical specialties ACUTE CARE COMMON STEM ACCS CT1 and CT2 6/12 Emergency Medicine 6/12Acute Medicine 6/12Anaesthetics 6/12 Intensive Care Medicine MCEM A/B/C MRCP I/II FRCA, ICM Exams Competitive Entry to ST1 ACCS from FY2/ equivalent by Interviews and streaming to specialty FY2 FY1
Post-CCT FCEM: SAQ+OSCEs ST6 CCT route Sub-specialisation: PEM, PHEM + 1 Yr ICM: 2yrs An 6/12 ICM18/12 CESR-CP combine competences in HST+ Non-Train posts ST4, ST5, ST6 36 months in EM HST 3-yrs MCEM: Part A +B: I, II ST3 EM PEM Paediatrics and further EM ACCS ST2 1 year Anaesthetics + ICU 6/12 each or 9/3 ST1 1 year EM + AM 6/12 each Core Training 3 yrs 2+3+3=8 Competitive Entry: ST1 ACCS (EM) +ST3 FY2 FY1 Foundation Training Run-through EM training 2015 CCT CCT EM +/- Sub-specialist – Independent specialist practitioner CA: ST3+ CTR =QIP Mg=Portfolio OOPs: T, E, R, B School of Emergency Medicine
ACCS: EM/AM, Anaesthetics/ITU Rotations • Norfolk/Suffolk 4 hosp • Cambridgeshire 4 • Beds/Herts 4 • Essex 5
ACCS CT1 year: Expectations • Emergency Medicine -- 6 months • Acute Medicine – 6 months (9/3 set up at AH) • Curriculum: induction pack what to cover • Simulation course: X3 AH • Life Support courses and teaching -GIC • Audits and presentations • Exams • MSF
What you’ll see in A&E…. • Acute medicine -lots • Paediatrics • Fractures • Minor injury • Primary care • Major trauma • O&G • Acute psychiatric • Acute surgery The College of Emergency Medicine
e-portfolios • EM and AM support both years of ACCS • RCoA only ACCS CT2 • CS and ES Report forms • WPBAs must do CT1 • ARCP Form
Supervision • Educational Supervisor for whole year • Usually from stream specialty • Initial meeting, mid-point end of year • ES structured report • Clinical Supervisor: each post 6/12 • Initial meeting, mid-point, end of 6/12 • CS report
EM WPBAs: 2015 curriculum Total 27 • CMP1 - Anaphylaxis • CMP2 – Cardio-respiratory arrest • CMP3 - Major Trauma • CMP4 - Septic patient • CMP5 - Shocked patient • CMP6 - Unconscious patient • CAP7 - Chest pain • CAP1 - Abdominal pain • CAP6 - Breathlessness • CAP30 - Mental health
AM: Minimum number of assessments per 6 months • 3 Mini-CEX • 5 DOPs • 3 Cbds • 3 ACATs plus 1 MSF
AM DOPs: • Lumbar puncture • Pleural tap & aspiration • Intercostal drain insertion (seldinger) • Intercostal drain insertion open • Ascitic tap • Abdominal paracentesis • DC cardioversion • Knee aspiration • Temporary pacing (external/wire) • Large joint examination
ACCS CT2 year • Anaesthetics –6/12 • Intensive Care Medicine –6/12 • Initial Assessment of Competence 3/12 • WPBAs • Log-Book • As per CT1: LSCs, Audit, MSF, Exams,
After ACCS: 3rd year • Anaesthetics –12/12 Total of 2 yrs before HST-ST3 • EM: The CT3 year: EM+PEM • AM: Additional year of Medicine: Ologies • Intensive Care Medicine –12/12
The ARCP Annual Review of competency and progressionAnnual Appraisal +Revalidation An Overview
Purpose of the ARCP Normally at least annually • A review and record of the trainee’s progress • Allows judgement to be made about the competences acquired by a trainee and their suitability to progress to the next stage of training • Provides final statement of trainee’s successful attainment of the competences and thereby completion of the training programme
ARCPs Applicable To: • All specialty trainees and core trainees • Academic trainees • Trainees OOP • LTFT trainees • FTSTAs • LATs
Basic Requirements • ES Structured report +CS reports • WpBAS • Curriculum covered • MSF: minimum 10 people of different grades/groups • Audit • Complaints/compliments/critical incidents • Enhanced Form R • All these organised through out the year
ARCP Checklist: • Up-to-date Curriculum Vitae • Completed and updated enhanced Form R • Structured Educational Supervisor • Clinical Supervisor report for each post – one form to be completed for each placement • Registration with the relevant College • WPBAs: See separate document for ARCP requirements for each post in ACCS programme • DOPS, CEX, CbDs, ACAT or ECAT • ALS ATLS EPLS APLS prn
ARCP Checklist: • Multi-Source Feedback: minimum 10 mix grades • Evidence of internal teaching attendance • Evidence of external courses and attendance • Evidence of audit or change management projects • Evidence of research and publications undertaken • List of sick, carer, paternal or maternity leave taken • Level two child protection training certificate • Evidence of compliments and thanks • Personal complaints received + any reflective notes • Personal concerns including Incidents reported, SUIs, any reflective notes
The Invitation to the Trainee • Must be sent at least 6 weeks before the ARCP • Reminds them that they need to get an educational supervisors report • Reminds them to update their CV • Reminds them about the relevant JRCPTB Decision Aid(s) and sends them the link(s)
Reminder to Trainees • A reminder about the ARCP is sent if they do not reply within 10 days • The Deanery does not check the eportfolios for Educational Supervisors reports or send reminders about these (not recommended in the Gold Guide)
The Day of the ARCPs The panel convene 15-30 minutes before ARCP agree: • Who will chair the panel • Who will complete the electronic and the handwritten records • Who will feedback to the trainee, including their training needs
ARCPs – The Procedure The eportfolio should be reviewed before inviting the trainee into the room: • Previous ARCP(s) • The educational supervisors report • The specialty curriculum, the GIM curriculum if appropriate (‘plenty of yellow, green and brown’) • Assessments, especially MSF.
Assessments • Generally formative • Try to ensure that they are done by appropriate people • The MSF can be valuable
ARCPs – The Procedure (3) The trainee is then invited into the room • Welcomed, panel members introduced • Purpose of ARCP explained • Outcome discussed (aim to be positive, supportive) • CCT date reviewed and if appropriate, Period of Grace discussed (entered in comments section on ARCP proforma in eportfolio) • Training to date and training needs discussed
Outcome 1 Satisfactory progress Fulfils all of the criteria of curriculum requirements
Outcome 2 Development of specific competences required – additional training time not required • Acceptable progress • Some competences not achieved • Not expected that overall progress (and therefore the CCT date) will be delayed • The trainee can ask for this outcome to be reviewed but cannot appeal
Outcome 3 Inadequate progress by the trainee – additional training time required • The panel considers that a period of additional training is required which will extend the duration of training • If this outcome is likely the trainee must be present. • The panel gives recommendations about the additional training. The Deanery decides the details, based on the panel’s recommendations • Usual maximum 1 year • The trainee can appeal
Outcome 4 Released from training programme with or without specified competences • Insufficient and sustained lack of progress, despite additional training • Panel should ensure that competences that have been achieved are documented • Trainee required to give up their NTN • The trainee can appeal
Outcome 5 Incomplete evidence presented – additional training time may be required • Examples include absent educational supervisor’s report, insufficient assessments, insufficient competences signed off • The trainee should submit a written explanation to the panel within 5 working days • The panel can require trainee to submit the necessary documentation by a designated date • Once documentation received, the panel can issue an assessment outcome (they don’t have to meet)
Outcome 6 Gained all required competences – will be recommended as having completed the training programme and for award of a CCT (or CESR)
Outcome 7 FTSTAs or LATs • The panel should give this outcome to FTSTAs and LATs, documenting the competences achieved
Outcome 8 Out of programme for research, approved clinical training or a career break • If the trainee is on a clinical placement, which has been prospectively approved by the GMC/PMETB, the usual documents for a clinical placement should be reviewed • If the trainee is in research the panel should receive a research supervisors report
Outcome 9 Doctors undertaking top-up training in a training post • Applies to doctors applying for a CESR where the GMC has recommended top-up training and they have been appointed competitively to a gap in a training programme. • The panel consider evidence including assessments to decide whether the objectives set by the GMC have been met
Trainees with an Adverse Outcome (2,3,4) Supplementary documentation should be completed by the ARCP panel and made available to: • The trainee • TPD • Educational supervisor • Medical director and Trust HR department • JRCPTB
Enhanced Form R: and Revalidation • Scope of practice: current jobs, • Other work: locums, volunteer work, formal teach • Revalidation officer: Prof Simon Gregory • Revalidation Date from GMC • Complaints/complements • Incidents, Adverse Events • Reflection on these • Probity: nothing to declare? • Concerns for revalidation • Any concerns from ARCP reported to PG Dean
Out of Programme - Research Documentation required: • OOPR return • Report from research supervisor This should indicate whether appropriate progress has been made with the research and ‘that the planned date of completion.. has not changed’
Out of Programme - Research Duration of research: • Should not normally exceed 3 years • A request to exceed 3 years must be made by the research supervisor to the Dean at least a year in advance Outcome: • The panel should issue an OOP outcome, recommending continuation of the OOPR or it’s termination, with a date
Less Than Full Time Training • LTFT trainees should still have ARCPs annually • Important to review CCT date carefully taking into account LTFT training
Simulation Addenbrooke’s Hospital • X 3 a year • X10 each course • Get in touch with PGC AH: Sue East