Download
1 / 46
490 likes | 807 Views
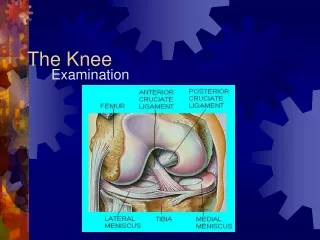
The knee. Mark Clathworthy, Patrick Djian, Bjorn Engstrom, Bent Wulff Jakobsen. Contents. Position of the patient Standard portals anatomy Additional portals Routine travel through knee Supra patellar pouch Patello femoral joint Medial gutter Medial compartment Intercondylar notch

E N D
The knee. Mark Clathworthy, Patrick Djian, Bjorn Engstrom, Bent Wulff Jakobsen
Contents Position of the patient Standard portals anatomy Additional portals Routine travel through knee Supra patellar pouch Patello femoral joint Medial gutter Medial compartment Intercondylar notch Lateral compartment Lateral gutter Posterior cavity Variation of normal mediale plica anterior plica Take home message
Positioning of the patient Lat support Supine Prepared Draped
Tourniquet and irrigation • Pressure tourniquet 280-350 mmHg • Irrigation options: • Arthroscopic pump • Gravity • Pressure saline bags
Standard portals • Antero-lateral (1) • the a-l portal is used as the standard viewing portal, through which you can access most of the joint • Antero-medial (2) • the a-m portal is used as the standard working portal through which you can probe the majority of the joint • Superior-lateral (3) • The s-l portal is used for optional outflow cannula and for probing the suprapatellar cavity • Posterior-medial (4) • The p-m portal is used accessing the posterior cavity • Antero-lateral (1) • the a-l portal is used as the standard viewing portal, through which you can access most of the joint • Antero-medial (2) • the a-m portal is used as the standard working portal through which you can probe the majority of the joint • Superior-lateral (3) • The s-l portal is used for optional outflow cannula and for probing the suprapatellar cavity • Posterior-medial (4) • The p-m portal is used accessing the posterior cavity • Antero-lateral (1) • the a-l portal is used as the standard viewing portal, through which you can access most of the joint • Antero-medial (2) • the a-m portal is used as the standard working portal through which you can probe the majority of the joint • Superior-lateral (3) • The s-l portal is used for optional outflow cannula and for probing the suprapatellar cavity • Posterior-medial (4) • The p-m portal is used accessing the posterior cavity • Antero-lateral (1) • the a-l portal is used as the standard viewing portal, through which you can access most of the joint • Antero-medial (2) • the a-m portal is used as the standard working portal through which you can probe the majority of the joint • Superior-lateral (3) • The s-l portal is used for optional outflow cannula and for probing the suprapatellar cavity • Posterior-medial (4) • The p-m portal is used accessing the posterior cavity 3 1 2 2 4 Courtesy to Pao Golano Courtesy to Pao Golano
Anatomy The subcutaneous nerve around the knee of importance related to the arthroscopic portals is the infrapatellar branch of the saphenus nerve. The antero-medial portal is closely related to the branch. The antero-lateral portal is only related to subcutaneous nerve branches in cases of abnormal anatomical arrangement. The postero-medial portal is placed immediately proximal to the hamstring tendons thereby avoiding the nerve branch of the saphenus nerve and the vessels. The subcutaneous nerve around the knee of importance related to the arthroscopic portals is the infrapatellar branch of the saphenus nerve. The antero-medial portal is closely related to the branch. The antero-lateral portal is only related to subcutaneous nerve branches in cases of abnormal anatomical arrangement. The postero-medial portal is placed immediately proximal to the hamstring tendons thereby avoiding the nerve branch of the saphenus nerve and the vessels. The subcutaneous nerve around the knee of importance related to the arthroscopic portals is the infrapatellar branch of the saphenus nerve. The antero-medial portal is closely related to the branch. The antero-lateral portal is only related to subcutaneous nerve branches in cases of abnormal anatomical arrangement. The postero-medial portal is placed immediately proximal to the hamstring tendons thereby avoiding the nerve branch of the saphenus nerve and the vessels. The subcutaneous nerve around the knee of importance related to the arthroscopic portals is the infrapatellar branch of the saphenus nerve. The antero-medial portal is closely related to the branch. The antero-lateral portal is only related to subcutaneous nerve branches in cases of abnormal anatomical arrangement. The postero-medial portal is placed immediately proximal to the hamstring tendons thereby avoiding the nerve branch of the saphenus nerve and the vessels.
Additional portals • Middle patella medial (5) • Additional portal convenient for viewing anterior of medial meniscus • Middle patella lateral (6) • Additional portal convenient for viewing anterior horn of lateral meniscus • Postero-lateral (7) • Additional portal convenient for viewing and exploring postero-lateral compartment • Middle patella medial (5) • Additional portal convenient for viewing anterior of medial meniscus • Middle patella lateral (6) • Additional portal convenient for viewing anterior horn of lateral meniscus • Postero-lateral (7) • Additional portal convenient for viewing and exploring postero-lateral compartment • Middle patella medial (5) • Additional portal convenient for viewing anterior of medial meniscus • Middle patella lateral (6) • Additional portal convenient for viewing anterior horn of lateral meniscus • Postero-lateral (7) • Additional portal convenient for viewing and exploring postero-lateral compartment 6 5 7 Courtesy to Pao Golano
Routine knee arthroscopy • Left knee
1. Insert the blunt trocar through the antero-lateral to the patello femoral pouch. Attach 30° arthroscope and look through suprapatellar pouch by rotating the scope 180° back and forward and scan the area. 2. Pull back gently scope overlooking patellofemoral joint on the extended knee from lateral and from medial side. If you drain the joint you can examine the patellofemoral joint stability better. 3. Reopen water supply and return to suprapatellar pouch. Follow capsular fold medial through the medial gutter to overlook the synovium and the medial femoral condyle. 4. Note the anterior horn of the med meniscus and apply a gentle valgus load on the lower leg to open medial compartment. Mark externally the spot for the medial portal with finger on skin or with a needle. 1. Insert the blunt trocar through the antero-lateral portal to the patello femoral pouch. Attach 30° arthroscope and look through suprapatellar pouch by rotating the scope 180° back and forward and scan the area. 2. Pull back gently scope overlooking patellofemoral joint on the extended knee from lateral and from medial side. If you drain the joint you can examine the patellofemoral joint stability better. 3. Reopen water supply and return to suprapatellar pouch. Follow capsular fold medial through the medial gutter to overlook the synovium and the medial femoral condyle. 4. Note the anterior horn of the med meniscus and apply a gentle valgus load on the lower leg to open medial compartment. Mark externally the spot for the medial portal with finger on skin or with a needle. 1. Insert the blunt trocar through the antero-lateral portal to the patello femoral pouch. Attach 30° arthroscope and look through suprapatellar pouch by rotating the scope 180° back and forward and scan the area. 2. Pull back gently scope overlooking patellofemoral joint on the extended knee from lateral and from medial side. If you drain the joint you can examine the patellofemoral joint stability better. 3. Reopen water supply and return to suprapatellar pouch. Follow capsular fold medial through the medial gutter to overlook the synovium and the medial femoral condyle. 4. Note the anterior horn of the med meniscus and apply a gentle valgus load on the lower leg to open medial compartment. Mark externally the spot for the medial portal with finger on skin or with a needle. 1. Insert the blunt trocar through the antero-lateral portal to the patello femoral pouch. Attach 30° arthroscope and look through suprapatellar pouch by rotating the scope 180° back and forward and scan the area. 2. Pull back gently scope overlooking patellofemoral joint on the extended knee from lateral and from medial side. If you drain the joint you can examine the patellofemoral joint stability better.. 3. Reopen water supply and return to suprapatellar pouch. Follow capsular fold medial through the medial gutter to overlook the synovium and the medial femoral condyle. 4. Note the anterior horn of the med meniscus and apply a gentle valgus load on the lower leg to open medial compartment. Mark externally the spot for the medial portal with finger on skin or with a needle. 1. Insert the blunt trocar through the antero-lateral portal to the patello femoral pouch. Attach 30° arthroscope and look through suprapatellar pouch by rotating the scope 180° back and forward and scan the area. 2. Pull back gently scope overlooking patellofemoral joint on the extended knee from lateral and from medial side. If you drain the joint you can examine the patellofemoral joint stability better. 3. Reopen water supply and return to suprapatellar pouch. Follow capsular fold medial through the medial gutter to overlook the synovium and the medial femoral condyle. 4. Note the anterior horn of the med meniscus and apply a gentle valgus load on the lower leg to open medial compartment. Mark externally the spot for the medial portal with finger on skin or with a needle. Routine travel 1 3 8 2 9 10 5 4 7 6
5. Rotate the scope looking centrally while flexing the knee to 90° examining the anterior cruciate from distally to proximally carefully probing the femoral attachment site. Next rotate the scope more medial to check the posterior cruciate often covered with synovium. 6. Rotate the scope looking laterally while applying a light varus stress to the slightly flexed knee – thereby overlooking and probing anterior horn of the lateral meniscus. Go to the ”figure of 4” position while keeping the scope parallel to tibial surface overlooking the middle third and posterior horn of meniscus. 7. Extend the knee and go directly to the lateral gutter, flex the knee and examíne the popliteus tendon and hiatus. 5. Rotate the scope looking centrally while flexing the knee to 90° examining the anterior cruciate from distally to proximally carefully probing the femoral attachment site. Next rotate the scope more medial to check the posterior cruciate often covered with synovium. 6. Rotate the scope looking laterally while applying a light varus stress to the slightly flexed knee – thereby overlooking and probing anterior horn of the lateral meniscus. Go to the ”figure of 4” position while keeping the scope parallel to tibial surface overlooking the middle third and posterior horn of meniscus. 7. Extend the knee and go directly to the lateral gutter, flex the knee and examíne the popliteus tendon and hiatus. Routine travel 5. Rotate the scope looking centrally while flexing the knee to 90° examining the anterior cruciate from distally to proximally carefully probing the femoral attachment site. Next rotate the scope more medial to check the posterior cruciate often covered with synovium. 6. Rotate the scope looking laterally while applying a light varus stress to the slightly flexed knee – thereby overlooking and probing anterior horn of the lateral meniscus. Go to the ”figure of 4” position while keeping the scope parallel to tibial surface overlooking the middle third and posterior horn of meniscus. 7. Extend the knee and go directly to the lateral gutter, flex the knee and examíne the popliteus tendon and hiatus. 1 3 8 2 10 9 5 4 7 6
8. Return to the ”figure of 4” position guiding the movement with the scope centrally in the notch looking laterally. Rotate the scope while probing the lateral meniscus. Note popliteus tendon above and below the meniscus runnning though the popliteus hole. 9. While in the ”figure of 4” position mark the triangular shape given from lateral femoral condyle, tibial plateau and anterior cruciate. Looking parallel to the tibial plateau pass gentle the scope through the triangle to the posterior cavity. Check posterior horn of lateral meniscus, posterior cavity by rotating the the scope 360°. Retract the scope while overlooking the posterior cruciate and the proximal part of the anterior cruciate. Routine travel 8. Return to the ”figure of 4” position guiding the movement with the scope centrally in the notch looking laterally. Rotate the scope while probing the lateral meniscus. Note popliteus tendon above and below the meniscus runnning though the popliteus hole. 9. While in the ”figure of 4” position mark the triangular shape given from lateral femoral condyle, tibial plateau and anterior cruciate. Looking parallel to the tibial plateau pass gentle the scope through the triangle to the posterior cavity. Check posterior horn of lateral meniscus, posterior cavity by rotating the the scope 360°. Retract the scope while overlooking the posterior cruciate and the proximal part of the anterior cruciate. 1 3 8 2 9 10 5 4 7 6
10. Put the knee 90 degrees of flexion. There will then be a triangle given from the medial femoral condyle, tibialplateau and the anterior cruciate ligament. Looking parallel to the tibial plateau pass gently the scope through the triangle to the posterior cavity. Sometimes you need to push the cruciate ligaments laterally and rotate the scope smoothly to pass this area. Check the posterior horn of the medial meniscus, posterior cavity by rotating the scope 360 degrees. Retract the scope while overlooking the posterior cruciate. Routine travel 1 3 8 2 9 10 5 4 7 6
10 Supra patellar pouch • Superior view of supra patellar pouch; 30° arthroscope 1 7 3 8 2 9 5 4 6
10 Supra patellar pouch • Superior view of supra patellar pouch; 30° arthroscope Vastus lateralis of the quadriceps muscle 1 7 3 8 2 9 5 4 6
1 7 3 8 2 10 9 5 4 6 Patello femoral joint • Femoral condyle lateral view; 30° arthroscope Femoral condyle lateral
1 7 3 8 2 10 9 5 4 6 Patello femoral joint Patello femoral joint • Femoral trochlea lateral view; 30° arthroscope Femoral trochlea
1 7 3 8 2 10 9 5 4 6 Patello femoral joint Patella • Patello femoral joint proximal lateral view; 30° arthroscope Femoral trochlea
1 7 3 8 2 10 9 5 4 6 Medial gutter Patella • Medial view of medial gutter; 30° arthroscope Medial femoral condyle Gutter
1 7 3 8 2 10 9 5 4 6 Medial gutter • Medial distal view of medial gutter; 30° arthroscope Medial femoral condyle Gutter
1 7 3 8 2 10 9 5 4 6 Medial compartment Medial femoral condyle • Distal view of medial meniscus anterior horn, knife producing a-m portal; 30° arthroscope Medial meniscus Knife in a-m portal Tibial plateau
1 7 3 8 2 10 9 5 4 6 Medial compartment • Distal view of medial meniscus anterior horn, probe through ant-med portal; 30° arthroscope Medial femoral condyle Tibial plateau Medial meniscus
1 7 3 8 2 10 9 5 4 6 Medial compartment Medial meniscus, undersurface Medial femoral condyle • Antero medial view of medial meniscus anterior horn underside, probe through ant-med portal; 30° arthroscope Tibial plateau
1 7 3 8 2 10 9 5 4 6 Medial compartment Medial femoral condyle • Medial view of medial meniscus central third; 30° arthroscope Medial meniscus Tibial plateau
1 7 3 8 2 10 9 5 4 6 Medial compartment Medial femoral condyle • Medial view of medial meniscus central third, probe through anteromedial portal; 30° arthroscope Medial meniscus Tibial plateau
1 7 3 8 2 10 9 5 4 6 Medial compartment Medial femoral condyle • Posteromedial view of medial meniscus posterior horn; 30° arthroscope Medial meniscus Tibial plateau
1 7 3 8 2 10 9 5 4 6 Medial compartment Medial femoral condyle • Posteromedial view of medial meniscus posterior horn, tested with a probe; 30° arthroscope, Medial meniscus Tibial plateau
1 7 3 8 2 10 9 5 4 6 Medial compartment • Inferomedial view of anterior part of joint, femoral condyles, trochlea and Hoffa’s fat; 30° arthroscope Medial femoral condyle
1 7 3 8 2 10 9 5 4 6 Intercondylar notch • Inferior view of distal tibial attachment of anterior cruciate ligament, knee near extension; 30° arthroscope Lateral femoral condyle Anterior cruciate
1 7 3 8 2 10 9 5 4 6 Intercondylar notch Posterior cruciate • Postero-central view of distal tibial attachment of anterior cruciate ligament, knee flexed 80°; 30° arthroscope Lateral femoral condyle Anterior cruciate
1 7 3 8 2 10 9 5 4 6 Intercondylar notch Lateral femoral condyle Anterior cruciate Postero-central view of proximal femoral attachment of anterior cruciate ligament; 30° arthroscope
1 7 3 8 2 10 9 5 4 6 Intercondylar notch • Postero-central view of posterior cruciate, knee flexed 80°, PCL covered with synovium; 30° arthroscope Posterior cruciate Anterior cruciate
1 7 3 8 2 10 9 5 4 6 Intercondylar notch • Postero-central view of posterior cruciate, knee flexed 80°, PCL release from synovium; 30° arthroscope Posterior cruciate Medial femoral condyle Anterior cruciate
1 7 3 8 2 10 9 5 4 6 Lateral compartment • Anterior view of lateral meniscus anterior horn; 30° arthroscope Lateral meniscus
1 7 3 8 2 10 9 5 4 6 Lateral compartment Lateral femoral condyle Popliteus tendon • Antero-lateral view of lateral meniscus; 30° arthroscope Lateral meniscus
1 7 3 8 2 10 9 5 4 6 Lateral compartment Lateral femoral condyle • Antero-lateral view of lateral femoral condyle; 30° arthroscope Lateral meniscus
1 7 3 8 2 10 9 5 4 6 Lateral compartment Lateral femoral condyle • Postero-lateral view of posterior horn of lateral meniscus and popliteus hole; 30° arthroscope Popliteus tendon Lateral meniscus
1 7 3 8 2 10 9 5 4 6 Lateral gutter • Lateral view on lateral gutter; 30° arthroscope Lateral gutter
1 7 3 8 2 10 9 5 4 6 Lateral gutter • Lateral view on lateral gutter; 30° arthroscope Popliteus tendon Lateral femoral condyle Lateral meniscus
1 7 3 8 2 10 9 5 4 6 Lateral gutter • Lateral view on lateral gutter; 30° arthroscope Popliteus tendon Popliteus hole Lateral meniscus
1 7 3 8 2 10 9 5 4 6 Posterior compartment Medial femoral condyle • Medial view, scope along posterior cruciate to posteromedial pouch; 30° arthroscope Posterior horn Medial meniscus
1 7 3 8 2 10 9 5 4 6 Variation of normal Plica • Medial view of the medial plica; 30° arthroscope Medial femoral condyle Patella Medial femoral condyle Plica
1 7 3 8 2 10 9 5 4 6 Variation of normal • Posterolateral view of the anterior plica, ligamentum Mucosum; 30° arthroscope Medial femoral condyle Plica Anterior cruciate
1 7 3 8 2 10 9 5 4 6 Variation of normal • Postero lateral view of a discoid meniscus (this on 80% discoid); 30° arthroscope Lateral femoral condyle Discoid lateral meniscus
Take home points • Always mark the involved side and relevant anatomical structures. • Never use sharp trocars, always bluntly instruments. • Prior to surgery pressure the tourniquet at 350 mmHg on the involved upper leg, use gravity, pressure saline bags or arthroscopic pumps for irrigation. • Always perform an examination of the knee including stability testing prior to arthroscopy. • Start the arthroscopy with applying the antero-lateral portal and insert the scope along the lateral edge of the patella with the knee in extension and while lifting the patella. • Apply the following portals guided by the arthroscopic view, using a needle if convenient. • Always perform the arthroscopic evaluation of all parts of the knee before performing any arthroscopic surgery. • Always use a probe to examine menisci, joint cartilage and ligements while overlooking the different structures.
Questionnaire • What is the importance of the antero-lateral portal • Explain how to identify the antero-medial portal • Which subcutaneous nerve is at risk applying the antero-medial portal • Which anatomical structures are the landmarks when applying the postero-medial portal • What intraarticular structure should not be mistanken for the anterior cruciate ligament