Download
1 / 19
200 likes | 400 Views
Meningeal Release - Coccyx. What is it? Therapy localization Testing Correction Pelvic Floor. What is Meningeal Release?. The dura mater is firmly attached inside the cranial bowl, Atlas, Axis and third cervical by the filum terminale into the dorsum of the first coccygeal segment.

E N D
Meningeal Release - Coccyx • What is it? • Therapy localization • Testing • Correction • Pelvic Floor
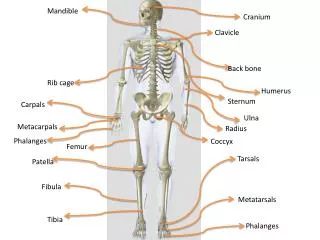
What is Meningeal Release? • The dura mater is firmly attached • inside the cranial bowl, • Atlas, Axis and third cervical • by the filum terminale into the dorsum of the first coccygeal segment
What is Meningeal Release? • In coccyx imbalances, abnormal stress can be applied to the dura mater causing reflex muscle tension along the spine. • Goodheart has described the coccyx as a take up mechanism to keep constant tension on the dura mater. • Tension on the dura appears to be controlled by the coccyx
Symptoms • Increased muscle contraction along the spine from the lumbars through the cervicals • Increased pterygoid pocket tenderness • Leg edema - tenderness • Visceroptosis • Dropped bladder - uterus • Open ICV
Spinal Length • Goodheart noted that healthy patients had the same spinal length, within 14 mm. (use rolling tape measure from coccyx to occiput) • If they were measured in the supine, sitting and standing positions. • Patient's with chronic problems have dramatic differences in the length of their spines.
Causes • “hemi-pelvis” • Fall on the pelvis • Cycling • Prolonged sitting with leg crossed • Child birth • Poor sitting posture
Therapy Localization • The patient is asked to therapy localize to the coccyx and apply inferior pressure. A strong muscle is tested for weakening. • Palpation of the paravertebral muscles will show tenderness on one side of the spine • Cervical paravertebrals are always present
Challenge • Palpate the associated muscle tenderness • Contact over the coccyx and traction the skin cephalad • Vary the vector until the greatest reduction in pain is found
Correction • Contact the skin over the coccyx and pull in the challenge direction found above. • Apply this pressure in a cephalad direction while the patient inspires. • Simultaneously, contact the atlas and pull inferior.
Repeat this five to seven times • Palpate for reduction in muscle tenderness • Remeasure the spinal length for normalization
Pelvic Floor • Test in cases of leg edema, increased venous pressure, obturator syndrome, general visceroptosis
Pelvic Floor • Tests are similar to the gluteus maximus starting position. • These were developed by Beardall • The leg is tested in a neutral position and with the leg internally and externally rotated 30 degrees
Pelvic Floor • If any of the three tests shows weakness • Challenge the coccyx for a position that strengthens the muscle • Correct in the challenge position
Coccygeus • Coccygeus is often described as the muscular belly of the sacrospinous ligament with which it is fused to on its pelvic aspect. • The coccygeus is occasionally absent, in which case the sacrospinous ligament is more prominent. • Proximal Attachment • This triangular sheet of muscle arises from the pelvic surface of the ischial spine and sacrospinous ligament.
Coccygeus • Proximal Attachment • This triangular sheet of muscle arises from the pelvic surface of the ischial spine and sacrospinous ligament. • Distal Attachment • Its base is attached to the lateral aspect of the coccyx and the fifth sacral segment.
Coccygeus Nerve Supply • A branch of the sacral plexus, derived from the ventral rami of S4 and S5 supplies coccygeus.
Coccygeus Action • The coccygeus muscle functions with the levator ani forming the majority of the pelvic diaphragm, which supports the pelvic viscera. • When the coccygeus and the levator ani contract with the muscles of the abdominal wall, they help to raise intra-abdominal pressure in such processes as coughing, vomiting and forced expiration. • They can also become involved in inspiration during respiration.
Sacrotuberous ligament • Has an extensive attachment; to the posterior superior and posterior inferior iliac spines, the posterior surface of the sacrum (where it blends with the posterior (dorsal) sacro-iliac ligaments), the lateral aspect of the lower sacrum and to the upper surface of the coccyx. • The fibers converge as they pass downwards and laterally. They twist on themselves and then diverge to attach to the medial margin of the ischial tuberosity and the lower margin of the ischial ramus. • Distal fibers of gluteus maximus attach to the ligaments posterior surface.