Download
1 / 60
600 likes | 870 Views
Heart Anatomy. Approximately the size of your fist Location Superior surface of diaphragm Left of the midline Anterior to the vertebral column, posterior to the sternum. Heart Anatomy. Figure 18.1. Coverings of the Heart: Anatomy.

E N D
Heart Anatomy • Approximately the size of your fist • Location • Superior surface of diaphragm • Left of the midline • Anterior to the vertebral column, posterior to the sternum
Heart Anatomy Figure 18.1
Coverings of the Heart: Anatomy • Pericardium – a double-walled sac around the heart composed of: • A superficial fibrous pericardium • A deep two-layer serous pericardium • The parietal layer lines the internal surface of the fibrous pericardium • The visceral layer or epicardium lines the surface of the heart • They are separated by the fluid-filled pericardial cavity
Coverings of the Heart: Physiology • The pericardium: • Protects and anchors the heart • Prevents overfilling of the heart with blood • Allows for the heart to work in a relatively friction-free environment
Pericardial Layers of the Heart Figure 18.2
Heart Wall • Epicardium – visceral layer of the serous pericardium • Myocardium – composed of aerobic muscle (contractile layer) • Composed of cardiac muscle bundles • Fibrous skeleton of the heart – crisscrossing, interlacing layer of connective tissue • Endocardium – endothelial layer of the inner myocardial surface • Lines the heart chamber and is continuous with the endothelial linings of the blood vessels
Left common carotid artery Brachiocephalic trunk Left subclavian artery Superior vena cava Aortic arch Right pulmonary artery Ligamentum arteriosum Left pulmonary artery Ascending aorta Left pulmonary veins Pulmonary trunk Left atrium Right pulmonary veins Auricle Right atrium Circumflex artery Right coronary artery (in coronary sulcus) Left coronary artery (in coronary sulcus) Anterior cardiac vein Left ventricle Right ventricle Great cardiac vein Marginal artery Anterior interventricular artery (in anterior interventricular sulcus) Small cardiac vein Inferior vena cava (b) Apex Figure 18.4b
Aorta Superior vena cava Left pulmonary artery Right pulmonary artery Left pulmonary veins Right pulmonary veins Auricle of left atrium Right atrium Left atrium Inferior vena cava Great cardiac vein Right coronary artery (in coronary sulcus) Posterior vein of left ventricle Coronary sinus Posterior interventricular artery (in posterior interventricular sulcus) Left ventricle Middle cardiac vein Apex Right ventricle (d) Figure 18.4d
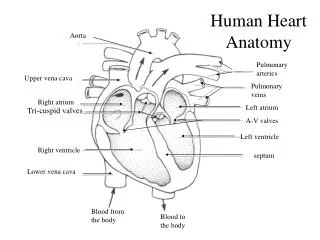
Aorta Superior vena cava Left pulmonary artery Right pulmonary artery Left atrium Pulmonary trunk Left pulmonary veins Right atrium Right pulmonary veins Mitral (bicuspid) valve Fossa ovalis Aortic valve Pectinate muscles Pulmonary valve Left ventricle Tricuspid valve Papillary muscle Right ventricle Chordae tendineae Interventricular septum Myocardium Trabeculae carneae Visceral pericardium Inferior vena cava Endocardium (e) Figure 18.4e
Atria of the Heart • Atria are the receiving chambers of the heart • Each atrium has a protruding auricle • Atria are relatively small, thin walled chambers • Atria contribute little to the propulsive pumping of the heart • Blood enters right atria from superior and inferior venae cavae and coronary sinus • Blood enters left atria from pulmonary veins
Ventricles of the Heart • Ventricles are the discharging chambers of the heart • Make up most of the volume of the heart • Trabeculae carnae are irregular ridges of myocardium • Papillary muscles are involved with valve function • Right ventricle pumps blood into the pulmonary trunk • Left ventricle pumps blood into the aorta
Pathway of Blood Through the Heart and Lungs • Right atrium tricuspid valve right ventricle • Right ventricle pulmonary semilunar valve pulmonary arteries lungs • Lungs pulmonary veins left atrium • Left atrium bicuspid valve left ventricle • Left ventricle aortic semilunar valve aorta • Aorta systemic circulation
Pathway of Blood Through the Heart • Pulmonary circuit is involved with gas exchange • Systemic circuit pumps oxygenated blood to the body • The two ventricles have unequal work loads • Right ventricle: short, low-pressure circulation • Left ventricle: long, high-pressure circulation, 5x more resistance than r. ventricle
Coronary Circulation • Blood in the heart provides little nourishment to the heart • Coronary circulation is the shortest circulation in the body • Provided by the r. & l. coronary arteries arising from the base of the aorta & encircling the heart in the coronary sulcus • These vessels lie in the epicardium and send branches inward towards the myocardium • Venous blood is collected by the coronary veins following the same path as the arteries leading to the coronary sinus and then the r. atrium
Coronary Circulation: Arterial Supply Figure 18.7a
Heart Valves • Heart valves ensure unidirectional blood flow through the heart • Atrioventricular (AV) valves lie between the atria and the ventricles & prevent backflow into the atria when ventricles contract • R. AV: tricuspid valve (3 cusps) • L. AV: bicuspid valve (2 cusps aka mitral valve) • Chordae tendineae anchor AV valves (in the closed position) to papillary muscles • Papillary muscles contract justpriorto ventricular contraction
Heart Valves • Aortic & pulmonary semilunar (SL) valves prevent backflow into the associated ventricles • Made of 3 cusps • Ventricular contraction forces valves open • Backflow fills the cusps thus moving (and closing them) backward • Due to low back pressure, they are not reinforced with cordae tendinae • Atrial contraction “pinches” off venae cavae and the pulmonary veins preventing substantial backflow through them
Heart Valves Figure 18.8a, b
Heart Valves Figure 18.8c, d
Atrioventricular Valve Function Figure 18.9
Semilunar Valve Function Figure 18.10
Microscopic Anatomy of Heart Muscle • Cardiac muscle is striated, short, fat, branched, and interconnected • Contracts via the sliding filament mechanism • Connective tissue is found in the intercellular space • The connective tissue endomysium is connected to the fibrous skeleton and acts as both tendon and insertion • The plasma membrane of adjacent muscle fibers interlock at intercalated discs • The discs contain anchoring desmosomes & gap junctions • Cardiac cells are electrically coupled through these gap junctions • 30% of the cell volume is mitochondria • 70% of the cell is myofibrils containing typical sarcomeres
Microscopic Anatomy of Cardiac Muscle Figure 18.11
Cardiac Muscle Contraction • Heart muscle: • Is stimulated by nerves and is self-excitable (automaticity) • Contracts as a unit • Has a long (250 ms) absolute refractory period (skeletal muscle = 1-2 ms)
Cardiac Contraction • Cardiac muscle contraction is similar to skeletal muscle contraction: • Depolarization opens a few fast voltage-gated Na+ channels • Presence of T-tubules • Ca++, troponin binding, sliding myofilaments • Cardiac muscle contraction differs from skeletal muscle contraction by: • Sarcoplasmic reticulum Ca++ release: • 20% Ca++ from extracellular space (slow Ca++ channels) • 80% Ca++ from S.R. • K+ permeability decrease preventing rapid repolarization • As long as Ca++ is entering, contraction continues • After 200ms, Ca++ channels close and K+ channels open
Heart Physiology: Intrinsic Conduction System • Autorhythmic cells: • Initiate action potentials • Have unstable resting potentials called pacemaker potentials • Use calcium influx (rather than sodium) for rising phase of the action potential
Energy & Electrical Requirements • The heart relies exclusively on aerobic respiration • Will use glucose and fatty acids, whichever is available • The heart does not rely on the nervous system to contract • However, autonomic nerve fibers can alter the basic rhythem • Setting the basic rhythem: Intrinsic Conduction System: • Presence of gap junctions • “In house” conduction • Consists of non-contractile cardiac cells that initiate and distribute impulses throughout the heart
Action potential Initiation by Autorhythmic Cells • Autorhythmic cells do not maintain a stable resting membrane potential • Rather, they continuously depolarize drifting towards threshold initiating the action potential • This is due to ion channels in the sarcolemma
Action potential Initiation by Autorhythmic Cells • Hyperpolarization closes K+ channels and opens slow Na+ channels • At 40 mV, Ca++ channels open producing the rising phase of the action potential and reversal of the membrane potential • Repolarization, as in skeletal muscle, reflects an increase in K+ permeability and efflux from the cell
Pacemaker and Action Potentials of the Heart Figure 18.13
Cardiac Membrane Potential Figure 18.12
Heart Physiology: Sequence of Excitation • 1) Sinoatrial (SA) node (located in the r. atrium) generates impulses about 75 times/minute • Sets pace for the heart as a whole (pacemaker) • 2) Atrioventricular (AV) node delays the impulse approximately 0.1 second • 3) Impulse passes from atria to ventricles via the atrioventricular bundle
Heart Physiology: Sequence of Excitation • 4) AV bundle splits into two pathways in the interventricular septum (bundle branches) • Bundle branches carry the impulse toward the apex of the heart 5) Purkinje fibers carry the impulse to the heart apex, ventricular walls, and papillary muscles Contraction begins at the apex and moves superiorly SA node: 75x/min (dominates) AV node: 50x/min AVbunde (Purkinje fibers): 30x/min
Cardiac Intrinsic Conduction Figure 18.14a
Cardiac Membrane Potential Figure 18.12
Heart Excitation Related to ECG SA node generates impulse; atrial excitation begins Impulse delayed at AV node Impulse passes to heart apex; ventricular excitation begins Ventricular excitation complete SA node AV node Bundle branches Purkinje fibers Figure 18.17
Extrinsic Innervation of the Heart • Heart is stimulated by the sympathetic cardioacceleratory center • Heart is inhibited by the parasympathetic cardioinhibitory center Figure 18.15
Extrinsic Innervation of the Heart • Cardiac centers are located in the medulla oblongata • Cardioacceleratory center projects to sympathetic neurons in the T1-T5 level of the spinal cord • Cardioinhibitory center sends impulses to the parasympathetic dorsal vagus nucleus in the medulla
Electrocardiography • Electrical activity is recorded by electrocardiogram (ECG) • Electrical currents generated in the heart spread throughout the body • 3 waves (deflections) • P wave corresponds to depolarization of SA node thru the atria. • QRS complex corresponds to ventricular depolarization • T wave corresponds to ventricular repolarization • Atrial repolarization record is masked by the larger QRS complex • P-Q interval is the time from the beginning of atrial excitation to the beginning of ventricular excitation • S-T segment is the time when the ventricle is depolarized • Q-T interval is the beginning of ventricular depolarization thru ventricular repolarization
Electrocardiography Figure 18.16
Heart Sounds • Two sounds can be distinguished when the thorax is ausculated (listened to) w/ stethescope • They are associated w/ the closing of heart valves • First sound occurs as AV valves close and signifies beginning of systole • Second sound occurs when SL valves close at the beginning of ventricular diastole
Heart Sounds Figure 18.19
Cardiac Cycle • Cardiac cycle refers to all events associated with blood flow through the heart • Systole – contraction of heart muscle • Diastole – relaxation of heart muscle
Phases of the Cardiac Cycle • Ventricular filling – mid-to-late diastole • Heart blood pressure is low as blood enters atria and flows into ventricles • AV valves are open but drift to closed position as blood fills ventricle (80%) • Atrial systole fills remaining 20% of ventricle • Atrial systole: depolarization (P-wave) • Atria contract, rise in atrial pressure • Ventricle in final part of diastole phase • Atrial diastole • Ventricles depolarize (QRS complex)
Phases of the Cardiac Cycle • Ventricular systole • Atria are in diastole • Ventricles begin contracting • Rising ventricular pressure results in closing of AV valves • Ventricular ejection phase opens semilunar valves
Phases of the Cardiac Cycle • Early diastole (following T wave • Ventricles relax • SL valves close w/ backflow from aorta and pulmonary arteries • When blood pressure on the atrial side excedes that in the ventricles, the AV valves open and ventricular filling begins again
Phases of the Cardiac Cycle • Notes: • Blood flow thru the heart is controlled totally by pressure changes • Blood flows down pressure gradients toward the lower pressure • Right side is low pressure • Left side is high pressure
Cardiac Output (CO) and Reserve • CO is the amount of blood pumped by each ventricle in one minute • CO is the product of heart rate (HR) and stroke volume (SV) • HR is the number of heart beats per minute • SV is the amount of blood pumped out by a ventricle with each beat • Cardiac reserve is the difference between resting and maximal CO
Cardiac Output: Example • CO (ml/min) = HR (75 beats/min) x SV (70 ml/beat) • CO = 5250 ml/min (5.25 L/min)
Regulation of Stroke Volume • SV = end diastolic volume (EDV; fill) minus end systolic volume (ESV; contraction) • EDV = amount of blood collected in a ventricle during diastole • ESV = amount of blood remaining in a ventricle after contraction