Download
1 / 29
310 likes | 530 Views
Detection of Mycobacterium Tuberculosis in Human Serum. Presented by: Thamir Alandijany Supervised by : Dr.Ahmad Al-Ghamdi. Introduction: Materials & Methods: Results Conclusion. Outline:. Tuberculosis.

E N D
Detection of Mycobacterium Tuberculosis in Human Serum Presented by: Thamir Alandijany Supervised by : Dr.Ahmad Al-Ghamdi
Introduction: Materials & Methods: Results Conclusion Outline:
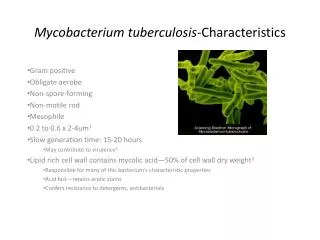
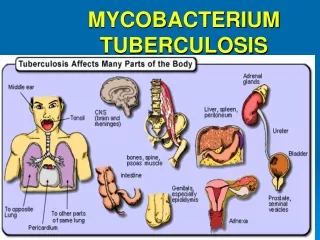
Tuberculosis • Tuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis: it affects mainly the lungs (pulmonary TB) but can attack any part of the body (extra pulmonary TB). (Runyon 1967). • Tuberculosis (TB) is a potentially fatal contagious disease. It is one of the the oldest disease known to mankind. Millions of new cases of TB occur each year world wide.
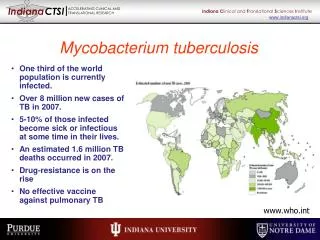
Incidence and Prevalence • Mycobacterial disease is one of the world's most difficult health problems. • One-third of the population worldwide is infected with TB. Of these, 8 to 10 million develop active disease and 2 million die each year. • It is the greatest cause of death in women of reproductive age; 9 million women are currently infected. Of these, 2.5 million will develop active disease and 1 million will die. (www.who.org). • One of the problems that face us in the treatment of tuberculosis is multi drug resistance tuberculosis (MDR TB) which was discovered In 1976 by David.
Mode of Transmission • The main rule of entry for the M. tuberculosis organism is the respiratory tract, TB infections are contracted by the airborne route, through the inhalation of droplet nuclei containing organisms of the tubercle bacillus from an infected individual.
Signs and symptoms • A person with inactive TB will have no symptoms. • A person with pulmonary TB may have any, all or none of the following symptoms: persistent, cough, weight loss, fever, loss of appetite, night sweats, shortness of breath and coughing up blood. • A person with extra-pulmonary TB may have the following general symptoms: Weight loss , Fever and Night sweats.
People at Risk of Tuberculosis • The risk of infection is high in close contact with a person with sputum positive pulmonary TB. • People with HIV infection, malnutrition and with uncontrolled diabetic patients (DM) are at high risk due to weakened immunity. • Intravenous drug abuse habit • Immunosuppressive therapy • Inadequate health care.
Diagnosis • Chest X-Ray • Tuberculin skin test • Laboratory diagnosis • Acid fast stain • Auramine-rhodamine flurochrome stain • Culture • Molecular methods • Serology: SD Rapid TB test
Are used to detect confluent granuloma formation in the lungs and possible cavitation, which could be a result of past or present infection with tuberculosis but it is almost impossible to make a diagnosis on this basis alone, because other diseases can mimic almost all of the manifestations of TB. Chest X-Rays
Tuberculin skin test • is performed to evaluate whether a person has been exposed to tuberculosis. If there has been a prior exposure, antibodies are formed and remain in the body. During the skin test, the tuberculosis antigen is injected under the skin and if antibodies are present, the body will have an immune response. There will be an area of inflammation at the site of the injection.
Acid fast stain • Ziehl-Neellsen and Kinyoun stain which use carbolfuchsin solution as primary stain, acid-alcohol as decolorizing agent and methylene blue as a counter stain. • Ziehl-Neelsen stain procedure involve the application of heat with carbolfuchin stain for better penetration of stain into the mycobacterial cell wall ,whereas the Kuinyoun acid fast stain is cold stain .
Auramine-rhodamine flurochrome stain • Fluorescence stain • More sensitive than carbolfuchsion stain.
Culture • Thereare a lot of Media used to grow M.tuberculosis, the most commonly used Media are: • Middle brook's medium which is a serum or agar based medium • Lowenstein-Jensen medium which is an egg based medium. • These media are incubated in 5-10% CO2 atmosphere to enhance growth require pH between 6.5-6.8 and it grow better at higher humidity. • M.tuberculosis colonies are small and buff colored when grown on either media. • Both types of media contain inhibitors to keep contaminants from out-growing M.tuberculosis. • It takes 4-6 weeks to get visual colonies on either type of media.
Molecular methods • Polymerase chain reaction (PCR) detects the bacterial DNA. Probes are now being used to aid in diagnosis of TB, with the benefit that fewer microbes need be present for positive identification .This type of testing can shorten diagnosis time to two days.
Serology • The One step SD Rapid TB test is a chromatographic immunoassay for the qualitative detection of antibodies to M.tuberculosis in human serum. • This test is intended for professional use as an aid in the detection of antibodies against M.tuberculosis in human serum. • Three specially selected TB recombinant proteins are used in test band as capture materials and gold conjugates. These enable the SD Rapid TB test to identify antibodies to TB in human's serum.
SD Rapid TB test device. 100ul micropipette. Centrifuge. Plane tube (red top) C T Materials
Collection of Samples • Twenty Blood samples of Tuberculosis patients were collected from King Abdulaziz Hospital and oncology center in Jeddah and Respiratory Diseases Hospital in Taif. • 14 of the samples were collected from males & 6 samples from females. • 5 samples from normal individuals were used as control.
Test Procedure & Result interpretation • Blood samples were collected in a plan tube (red top). • Blood sample was centrifuged at 4000 rpm for 5 minutes. centrifuge
C T Test Procedure & Result interpretation • A purple color is seen moving across the result window in the center of the device. • Results were interpreted at 15 minutes after sample application. • The test device was removed from the foil pouch, and placed on a flat and dry surface. • 100 uL of serum was added into the sample well (S) with micropipette.
C T Test Procedure & Result interpretation • Positive result: • Two strong pink-purple lines, one in each of the Control and Test areas. • One light pink-purple line in the Test area and one strong pink-purple line in the Control area.
C T Test Procedure & Result interpretation • Negative result: • Only one pink-purple line in the results window, in the Control area, with no distinctive pink-purple line in the Test area. This indicates that no active M. tuberculosis infection was detected.
C T Test Procedure & Result interpretation • Invalid result: • A distinct pink-purple line should always appear in the control area. The test is invalid if no line forms in the Control area regardless of the presence or absence of a line in the Test area.
Results • Seven out of the 14 samples (50%) which were collected from males, were positive for the SD rapid test. • One out of the 6 samples collected from females, was positive. • One out of the 5 samples collected from healthy individuals (control) was postive. • True positive samples: 8 • False positive samples: 1 • True negative samples : 6 • False negative samples: 10 • Sensitivity of kit: 44.4 % • Specificity of kit: 85.7 %
Conclusion • The SD rapid TB test is easy, simple, Qualitative & rapid but it isn’t reliable for Diagnosis of Tuberculosis because of low sensitivity . • False negative results were obtained with immunsuppresed (Immunocompremised) patients and TB patients with recent infection. • We recommend using large number of samples to examine the efficiency of the kit.