Download
1 / 80
980 likes | 1.22k Views
MYCOBACTERIUM TUBERCULOSIS. Introduction. Chronic granulomatous inflammation. Granuloma-granule like lesion Epithelioid cells,giant cells,necrosis & fibrosis. Factors favouring-poorly digestible irritant -cell mediated immunity. Causative organism.

E N D
Introduction • Chronic granulomatous inflammation. • Granuloma-granule like lesion • Epithelioid cells,giant cells,necrosis & fibrosis. • Factors favouring-poorly digestible irritant -cell mediated immunity.
Causative organism • Koch’s bacillus • Pathogenic strains -tuberculosis -bovis -avium -murine
Atypical mycobacteria-photochromogens -scotochromogens -nonphotochromogens -rapid growers. • Lesions caused-pulmonary -abscesses -lymphadenitis -bacteremia -ulcers -longer, thicker, more coarsely beaded, bent.
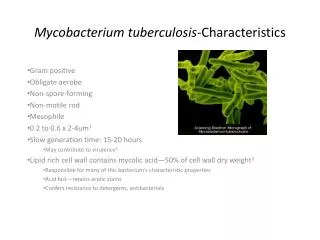
Mycobacterium TB • Slender, strictly aerobic rods • Waxy cell wall of mycolic acid • Methods of demonstration- -Ziehl-Neelsen method -fluorescent dye -culture-LJ medium -guinea pig inoculation
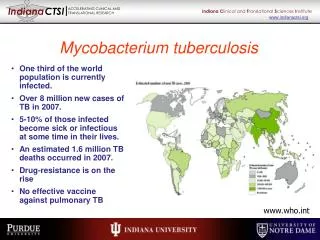
Epidemiology • 8 to 10 million cases/year • Leading infectious cause of death after HIV • Incidence increased after emergence of HIV • Flourishes-poverty,crowding,chronic debilitating illnesses,immunosuppression.
Modes of spread • Inhalation-airborne droplets • Ingestion-bovine TB • Inoculation - • Trans-placental- ?
Pathogenesis • Inhalation of tubercle bacilli • Mannose receptor of macrophage binds lipo-arabinomannan (LAM) on bacteria • Unchecked proliferation-?reasons • TH1 response-bactericidal macrophages • IFN gamma induces NO formation • TH1 response orchestrates formation of granuloma & caseous necrosis.
Tubercle • Caseous / non-caseous focus of inflammation consisting of : • Epitheloid cells • Langhan’s giant cells • Surrounded by lymphocytes and fibroblasts. • Fate of the tubercles– cold abscess, sinuses, coalesce to form large tubercles, dystrophic calcification.
Bacterial entry T Lymphocytes. Macrophages. Epitheloid cells. Proliferation. Central Necrosis. Giant cell formation. Fibrosis. TB Pathogenesis
Tubercle bacilli Lymphocyte Giant cells Fully activated macrophage Partially activated macrophage
Morphology of Granuloma • Rounded tight collection of chronic inflammatory cells. • Central Caseous necrosis. • Active macrophages - epithelioid cells. • Outer layer of lymphocytes & fibroblasts. • Langhans giant cells – joined epithelioid cells.
IFN gamma activates macrophages producing TNF • TNF recruits monocytes –epithelioid & giant cells • In summary - central role of TH1 -confers immunity -hypersensitivity- granuloma -caseation.
No infection 78% Exposure (close contact) Primary active TB 5% Continued latent TB Infection 22% Secondary TB 10%/lifetime Latent TB 95% HIV infection 10%/year Outcome of Exposure to M. tuberculosis
Primary tuberculosis: initial infection, usually in children - Ghon complex – sub-pleural granuloma + granulomatous hilar lymph node infection • Secondary tuberculosis: mostly in adults, reactivation of previous infection / reinfection. Granulomatous inflammation is much more florid and widespread - Typically, the upper lung lobes are most affected • Miliary tuberculosis- small millet seed (1-3 mm) sized granulomas
Types PRIMARY TB: -previously unexposed, unsensitized -exogenous source of infection -primary or Ghon complex a)primary Ghon focus b)lymphatic c)lymph node
2.PROGRESSIVE PRIMARY TB -resemble acute bacterial pneumonia -lower & middle lobe consolidation -hilar adenopathy -pleural effusion -cavitation rare 3.PRIMARY MILIARY TB -TB meningitis,miliary TB.
Fate of primary TB In 95% of cases healing by fibrosis -calcification -Ranke complex (X-ray)
SECONDARY TB: • Previously sensitized. • Re-activation of dormant bacilli • Re-infection TB A)high dose of virulent bacilli B)primary immunity wanes off.
Morphology • Initial lesion: -small focus(<2cm) of consolidation within 1-2 cms of apical pleura. -sharply circumscribed, firm ,grey-white to yellow areas with central caseation & peripheral fibrosis. -Because of good hypersensitivity ,walling off occurs.-FIBROCASEOUS SCARS.
PROGRESSIVE PULMONARY TB: -Elderly, Immunosuppression -apical lesion enlarges -erosion into a bronchus -ragged irregular cavity,poorly walled off Cavities may remain or collapse spread-airways, lymphatic, hematogenous
Miliary TB MILIARY PULMONARY DISEASE • Through lymphatics to Rt. side of heart and pulmonary arteries. • Small(2mm) yellow white consolidation scattered throughout lung. -Pleural spread -effusion -empyema -obliterative fibrous pleuritis.
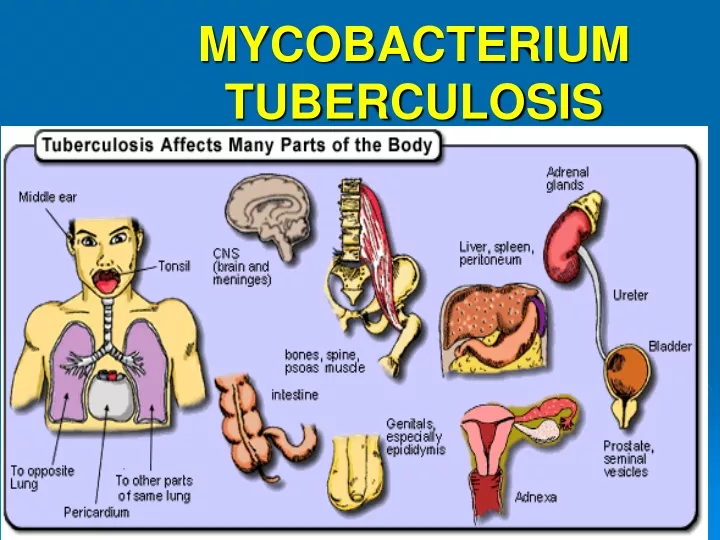
SYSTEMIC MILIARY DISEASE Hematogenous dissemination Organs affected: liver, spleen, kidneys, adrenals, bone marrow. Multiple tiny tubercles –grey white to yellow,
Endobronchial, endotracheal & laryngeal TB: • Infective material spread through lymphatics • Expectorated infectious material. • Mucosa studded with minute granulomas • Isolated organ TB & lymhadenitis are other forms of TB.
TB & HIV • Increased incidence in HIV • CD4 count >300 -secondary TB • CD4 count <200 -progressive primary • Sputum smear –ve, TUBERCULIN test –ve & rare formation of granulomas • Sheets of foamy histiocytes packed with bacilli.
In AIDS ,MAC causes widely disseminated infections • Proliferation in lungs & GIT • Fever, drenching night sweats & weight loss. • Enlargement of lymph nodes, liver & spleen • Granulomas, lymphocytes & tissue destruction are rare.
Clinical features • Malaise, anorexia, weight loss and fever • Low grade and remittent (appearing late each afternoon and then subsiding) • With progressive pulmonary involvement: increasing amounts of sputum, which is at first mucoid and later purulent may appear. • Haemoptysis • Pleuritic pain
Diagnosis History Clinical examination X-ray examination Smear for AFB Culture PCR