Download
1 / 43
430 likes | 465 Views
Gallbladder Disease. Gazi Rashid Lindsey Urquia. 5 Takeaways. Basic HPB layout and 2 important views during surgery Different types of gallstones and their risk factors Walk through an H&P & workup for acute cholecystitis Basics of Medical vs. Surgical mgmt for acute cholecystitis

E N D
Gallbladder Disease Gazi Rashid Lindsey Urquia
5 Takeaways • Basic HPB layout and 2 important views during surgery • Different types of gallstones and their risk factors • Walk through an H&P & workup for acute cholecystitis • Basics of Medical vs. Surgical mgmt for acute cholecystitis • Presentation and acute management of ascending cholangitis Extra: Recognize • Basic presentation & pathophys of gallstone ileus • Imaging & management of Porcelain GB • Surgical indications for asymptomatic cholelithiasis
Anatomy : Gazi - 5 min • Minor: Symp Chole, Choledocho, • Physiology/types of GS/risk factors: Lindsey - 5 min • GB pathology • Acute chole: Lindsey - 15 min • Patho → Pres • DDx • W/U – Labs, Imaging • Medical • Operative • Ascending chol : Gazi - 10 min • Patho → Pres (Triad, Pentad) • W/U → labs, imaging • Med/ICU mgmt • Operative/ERCP • Cases – core info (x3) - 10 min (6, 4) - I don’t know that we’ll have time to do 3 cases • Biliary colic-– Lindsey/Gazi + counseling • Acute Chole - 1 liner→ diagnosis: history/PE/labs/US/management - 5 Qs each - maybe include the “Pearls” here • Asc Chol - 5 review Qs, as this isn’t a typical H&P • Misc - Porcelain GB, Gallstone Ileus (5 min) • “pearls”– • Time for questions - 10-15 min (mention oral exams, resources to learn rest of biliary dz) • Appendix - at their own pleasure
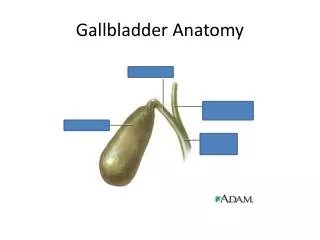
Anatomy Draw the hepatobiliary system - gallbladder, liver, pancreas, duodenum, and what connect them
Gallbladder • Cholelithiasis • Asymp. Vs Symp • Calculous Cholecystitis • Porcelain GB • Gallstone Ileus • Acalculous Cholecystitis • Gangrenous Cholecystitis • GB Carcinoma CDB - Choledocholithiasis - Ascending Cholangitis - Cholangiocarcinoma - Strictures from ERCP Cystic Duct - Mirizzi Syndrome Sphincter of Oddi Biliary Dyskinesia Cancer at the Head of the Pancreas
Critical View of Safety
Types of gallstones/risk factors • Biliary sludge – cholesterol crystals, Ca bilirubinate granules & mucin maxtrix • Impaired/slow contractility or bile stasis • Cholesterol (70-80%) • Most common • Increased ratio of chol:salts • Hormone (preg, OCP) • Pigmented (20-30%) • Bilirubin & calcium salts (20% cholesterol) • Cirrhosis, hemolytic anemia, hereditary spherocytosis
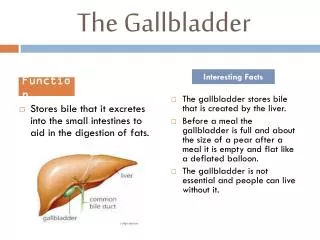
Acute cholecystitis • Pain – unrelenting right upper quadrant, midepigastric pain • Vs. Biliary colic • Nausea & vomiting • Fever/chills • Labs * - elevated enzymes/Br but relatively low • Obstruction of cyst duct from gallstone • 95% - calculi • 5% - acalculous (sludge) • GB continues to produce mucous ➔ distension ➔ venous congestion inflamed, edematous wall ➔ arterial inflow impaired ➔ stone dislodges (ischemia 5-10%)
Normal Gallbladder imaging
Acute Cholecystitis imaging
Acute Cholecystitis imaging
HIDA Scan(Hepatobiliary Iminodiacetic acid) If there’s a question…get a HIDA Highly sensitive & specific! (95%) imaging
Acute Cholecystitis imaging
Acute Cholecystitis medical mang • NPO • IV fluids • IV antibiotics • E. Coli, Klebsiella, Enterobacter, Bacteroides, Clostridium coverage • 2nd gen cephalosporin (cefoxitin) • Fluoroquinolones (Ciprofloxacin, Levofloxacin) • Ampicillin-sulbactam (Unasyn) • Surgery! treatment
Cholecystectomy • NPO, IVF, IV abx • Classic: Surgery safe if within 72 hours • Identify anatomical views & critical view • Intraoperative cholangiogram (IOC) – high suspicion for CBD stone • Lap > open conversion rate 0-20% treatment
Cholecystectomy treatment
Ascending cholangitis • Terms: Choledocholithiasis vs. Ascending Cholangitis • Acute Presentation (Charcot’s Triad): • Jaundice, RUQ pain, Fever • Complicated by Reynold’s pentad: Triad + Hypotension + AMS (Septic shock) • Not always due to stones!
Workup • Leukocytosis • Cholestatic Pattern of Liver Injury • ALP, GGT, Bilirubin >>> AST, ALT • All can be elevated • RUQ U/S: • Stone not always seen • Look for CBD dilatation
Management of Ascending Cholangitis • Mild ←→ Emergency! • Unstable patients: aggressive medical management, ICU • BP control:fluids, fluids, fluids • Monitoring • Blood cultures • Treatment: • IV broad spectrum antibiotics • Biliary decompression with ERCP (1st line) • Cholecystectomy when stable
Porcelain Gallbladder imaging
Gallstone Ileus • Misnomer! • Mechanical obstruction • Large impacted stone → Ischemia & pressure necrosis → Erosion into intestines→ cholecystic-enteric fistula • Bowel obstruction when stone is stuck at ileo-cecal valve
Gallstone Ileus Presentation • Elderly women with hx of biliary disease • Small bowel obstruction symptoms • N/V, diffuse abd pain, obstipation Imaging(plain films, CT scan) • Bowel obstruction findings: Air-fluid levels • Pneumobilia (gas in biliary tree) • Ectopic large gallstone
Case 1 42 y/o woman presents to clinic with abdominal pain 1. History – LOCATES 2. Physical exam 3. DDx 4. Labs 5. Management Bonus: What if this patient was asymptomatic and found – when would you do a cholecystectomy?
Case 1 • 42 y/o female with a 2 day history of RUQ & right upper back pain, assoc nausea. What’s your differential diagnosis? • Worse after meals. Similar episodes in the past. No f/c • Meds – OCP, MVI • PMH/PSH – HTN, hyperlipidemia, Lap gastric banding pathology
Acute Cholecystitis imaging
Diagnosis • History & physical exam • Ultrasound • 95% sensitive • Hyperechoic mobile densities within gallbladder with assoc hypoechoic shadowing diagnosis
Case 2 25 y/o female with a 2-day hx of fevers, chills, constant RUQ pain, scleral icterus, nausea, vomiting, BP 90/54, HR 117, T 39.1: • Next steps of management? • Other DDx? • Workup (Labs, Imaging, etc)? • What will 1st line imaging show? • What is the 1st-line therapeutic intervention? Describe it. Bonus: The pt.tells you that she’s had mouth sores & bloody diarrhea for months - what is the underlying pathology in this presentation?
Acute cholecystitis RUQ pain, nausea/vomiting, fever, increased WBC U/S (1st line): pericholecystic fluid, GB wall > 3mm thick, stones, sonographic Murphy’s HIDA 95% accurate Anatomy Modern Triangle of Calot: Cystic Artery, Hepatic Duct, Inf Liver Edge CVS: See cystic artery and cystic duct entering GB Acute cholangitis Charcot triad: (1) fever/chills + RUQ pain + jaundice Reynold’s pentad: Charcot’s triad + altered mental status + shock Emergency! Need ERCP summary
Symptomatic cholelithasis Intermittent RUQ pain, nausea, fever unlikely Diagnosis H&P, Ultrasound Gallstone Ileus 1 liner: Elderly women w/ SBO & history of biliary disease Transition point at ileocecal valve (stuck) Porcelain gallbladder Asymptomatic 25-50% assoc with gallbladder cancer summary
Case 2 • 79 y/o female with a 5 day history of diffuse abdominal pain, nausea, vomiting What’s your differential diagnosis? • Pain begin in RUQ, progressively worse, subjective chills • Meds – insulin, ASA • Pertinent hx – NH resident, diabetes pathology
Gallbladder Carcinoma • 0.5-1% of pop with cholelithiasis • Poor prognosis (unless T1a) • Most adenocarcinoma • Contracted (nondistended) • Risk Factors: adenomatous polyps, porcelain gallbladder (50%), biliary anomalies pathology
Gallbladder Carcinoma • Localized (lamina propria) • Cholecystectomy • Advanced Stage • radical cholecystectomy • Gallbladder + hepatic segments 4b & 5 + LND treatment
Mirrizzi Syndrome Common hepatic duct obstruction 2/2 impacted stone in cystic duct pathology
Biliary Dyskinesia • Impaired GB emptying or sphincter of Oddi relaxation • Biliary colic (post-prandial sharp RUQ pain), nausea • NO gallstones • Extensive w/u • HIDA + CCK • GB ejection fraction 35% or less pathology
Acalculous Cholecystitis • Seen in critically ill pt • Trauma • Burn • Prolonged TPN or NPO status (weeks) • Cardiopulmonary bypass • Often progress to gangrene or emphysematous cholecystitis • Fulminant course - has 40% mortality rate pathology
Imaging in Gallstone Ileus Imaging