Download
1 / 34
340 likes | 432 Views
MANAGEMENT OF HEALTH AND ENVIRONMENTAL RISKS: With a Case Study of Pandemic Influenza. Queen's Public Executive Program September 27 to October 9, 2009 William Leiss. William Leiss. Past-President, The Royal Society of Canada Officer, Order of Canada

E N D
MANAGEMENT OF HEALTH AND ENVIRONMENTAL RISKS:With a Case Study of Pandemic Influenza Queen's Public Executive Program September 27 to October 9, 2009 William Leiss
William Leiss • Past-President, The Royal Society of Canada • Officer, Order of Canada • Professor emeritus, School of Policy Studies, Queen's University • Scientist, McLaughlin Centre for Population Health Risk Assessment, University of Ottawa • Publications: www.leiss.ca • E-mail address: wleiss@uottawa.ca
Books on Risk Issues • I have been working in the risk studies field for over twenty years, primarily as a university-based researcher, but including consulting with Health Canada and for industry, especially the chemical industry • In 1994, I published Risk and Responsibility, with lengthy case studies in pesticides and EMF (electric and magnetic fields) risk
Books on Risk Issues (continued…) • William Leiss and Douglas Powell, Mad Cows and Mother's Milk: The Perils of Poor Risk Communication (1997) • It contains case studies of risk communication failures: Mad cow disease in the U.K., dioxins, "hamburger disease" (E. coli), silicon breast implants, bovine growth hormone, genetically-engineering food crops, and PCBs • Second edition with three new case studies (including BSE in North America), 2004
Books on Risk Issues (continued…) • Published 2001 • "Professional risk managers in governments and industry often completely misunderstand the nature of the reactions of the public to risks. Such misunderstandings are the initial steps which can, sometime later, help to cause the organizations they work for to stumble unwittingly into the labyrinth of risk controversy. Then the chamber of risks can turn into a chamber of horrors for business and governments."
Future Risks A Work of Utopian Fiction Book Two of The Herasaga Like priests, scientists are liable to be misled by the purity of their motives into downplaying the risks inherent in their creations. “It is, of course, quite correct for you to allot the relevant priesthood to Niels Bohr.” (Albert Einstein to Max Born, 7 September 1944) Book One is Hera, or Empathy Both from University of Ottawa Press or Amazon
Latest Book Forthcoming from The University of Ottawa Press in Spring 2010 Systemic Financial Risk by William Leiss Chapter I: Black Holes of Risk Chapter II:Systemic and Super-Systemic Risk in the Financial Sector Chapter III: Controlling the Downside
Overview Section A: Essentials of Good Risk Management Risk Management is the effort to anticipate and prevent or mitigate harms that may be avoidable.
What is Risk Management? Risk Assessment is the product of hazard and exposure: Hazard: The bad thing that could happen to someone. Exposure: Do you personally (or your family, etc.) have a risk factor that means that the bad thing could happen to you? Risk Factor: Activity that exposes someone to the hazard (smoking is a risk factor for lung cancer). Risk Estimation: Since you don't know if the bad thing will happen or not, you have to estimate [make an educated guess about] its likelihood and consequences. Risk Estimation: Probability x Consequences (R=P x C) Likelihood: probability of occurrence (% chance in a certain time-frame [smoking over an adult lifetime: about 20%] Consequence: How bad will it be for me, or many persons, if the bad thing does happen (lung cancer = premature death)?
What does Risk Management involve? The essence of effective risk management can be summed up in three “simple” directives: • Foresight: plan (don’t wait for the disaster to strike); • Precaution: insure or spend judiciously in advance; • Protect the Downside: whatever else you do, make sure you have limited the extent of the possible losses (“minimax” strategy, or “don’t bet the farm”). The banking and insurance industries invented all this, beginning in the 17th century; recent events suggest they have quite deliberately tried to ignore everything they ever knew (see Gillian Tett’s 2009 book, Fool’s Gold)
The Risk Management Approach • Perform a formal risk estimation [R=P x C] and assign a risk class (level of severity): • High-probability, low-consequence (ordinary flu, except for certain classes of people, e.g., elderly) • Low-probability, high-consequence (terror attack) • Specify the residual uncertainties • List the available risk control options, including: • feasibility • cost • public perception of risk • Evaluate options against objectives in the light of the risk estimation; • Make a decision, with an explicit rationale.
Understanding Uncertainty is Key • Two dimensions: Likelihood and Confidence.* • Likelihood: Qualitative and Quantitative Expressions (scale of10) Exceptionally unlikely <1% probability Very unlikely <10% probability Unlikely <33% probability About as likely as not 33-66% probability More likely than not >50% probability Very likely >90% probability Virtually certain >99% probability • Confidence: Qualitative (5-point scale): Very low confidence Less than 1 chance in 10 Medium confidence About 5 chances in 10 High Confidence About 8 chances in 10 *Intergovernmental Panel on Climate Change
Why Risks are Tricky Getting away with using hazardous materials Everything is hazardous at some dose. Where is the "safe" level of exposure? Examples: Lead and infants, medical X-rays Latency Hazard does not show itself clearly or soon enough: Lung cancer rates track smoking onset by 20 years. Only epidemiology can show this to us Confounding risk factors Asbestos or smoking? Answer: Both Relative risk Nicotine is more addictive than cocaine or heroin. So why is one a legal drug while the others are not? The "Golden Mean" Where is the crossover point for amount of wine consumption (from benefit to excess risk)? Alas, it seems to occur at a much lower level for women!
Risk-Management: Challenges • Citizens faced with exceedingly complex risk factors where science is confusing and unfamiliar (genetics, climate) • Citizens trying to figure out trade-offs between risks and benefits across multiple and dissimilar dimensions of everyday life (health, environment) • People trying to figure out whether someone is trying to pull the wool over their eyes, because they hear conflicting versions of events (climate, genetics) • BUT: Used properly, the risk approach can be a huge benefit right across the spectrum, from personal choices, to family choices, for governments and business, and for public policy generally
The Generality of Risk Management • Exactly the same 3-step approach, as described, should be used for all risks, including: • Financial sector regulation (the 2008 meltdown was a disaster waiting to happen); • Environmental risks, including climate change, nuclear waste, toxic chemicals, habitat protection, etc.; • Public health risks, including pandemic influenza, food- and water-borne pathogens, air quality, etc.; • “Private” health risk management, as undertaken by families and individuals (over 75% of lifetime health outcomes are determined by risk factors over which we have some control; • Teenagers and their parents (the teenage years represent the most significant risk scenario in a modern society); • Sub-populations at elevated risk, e.g., native peoples.
Case Studies Section B: Two Important Current Cases in Health Risk: Blood Safety and Pandemic Influenza Planning Both cases show us very clearly how unavoidable uncertainties in risk estimations can make risk management decision making both onerous and controversial. And yet, we have no better option than the practice of risk management when we are faced with the question: What should we do?
First Case Study Blood Safety • The responsibility of a federal agency, Canadian Blood Services (paid for by the provinces) • Blood used in medical applications is almost certainly safer now than it has ever been • But in recent history there were terrible cases of risk management failure (avoidable harm) • Caused Red Cross to lose its traditional mandate here
Risk Management of Donated Blood Canadian Blood Services indefinitely defers any male from donating blood if he answers yes to the question: "Have you had sex with a man, even one time since 1977?" "The basic premise for the deferral criteria is that the prevalence and incidence of HIV is much higher in males who have had sex with other males (MSM) than it is in individuals having exclusively heterosexual sex, according to 2005 statistics from the Public Health Agency of Canada."
Context • MSM donor deferral was put in place in the context of the great tragedies of the 1980s and 90s - infection of the supply of donated blood by HIV and Hepatitis C - and the responses by governments in North America, Europe, Japan and elsewhere, involving inquiries, criminal prosecutions, and huge changes to the institutional systems for blood safety • Mr. Justice Horace Krever, "Commission of Inquiry into the Blood System in Canada," 3 vols., 1997 • André Picard, The Gift of Death (1995)
MSM as a Risk Issue • The deferral policy for MSM is based on the notion of "excess risk" (2006 StatsCan data): • HIV prevalence: half of all cases occur in MSM • HIV Incidence (new cases): 45% are MSM • In Canada, est. 2% are gay/male bisexual • Trend for HIV prevalence in Canada: 16% increase since 2002 • Relative Prevalence Ratios (HIV/AIDS): • MSM: General population ~65:1 (Canada, StatsCan data) • MSM: New blood donors ~200:1 (U.S. estimate) 3. MSM: Repeat blood donors ~2000:1 (U.S. estimate)
Evidence from published studies • Accepting donations from MSM sexually abstinent for one year represents an increase in risk over the present deferral • MSM sexually abstinent for five year appear to present a risk no higher than heterosexuals, although a very small incremental risk cannot be ruled out • What should we do? • Leiss, Tyshenko & Krewski, "MSM Donor Deferral Risk Assessment: An Analysis using Risk Management Principles," January 2007: http://www.leiss.ca/index.php?option=com_content&task=view&id=98&Itemid=48 [published in Transfusion Medicine Reviews]
Conclusions • The good news is that the risks of the major Transfusion-Transmitted Infections are so low that they cannot be measured directly, but only estimated; • The bad news (for the public policy issues around MSM) is that one cannot tell whether making small adjustments to donor deferral policy represents an increase or decrease in actual (as opposed to estimated) risk. • Almost certainly, on the basis of the evidence we have, we could reduce the current lifetime deferral period to 5 years abstinent, without any increase in real risk. • Should this change be made?
Second Case Study Pandemic Influenza Planning
Pandemic Influenza Planning (Avian Flu) • PIP is an excellent illustration of all of the key points made earlier about Risk Management: • The structure: Foresight – Precaution – Protect the Downside; • The key role of managing uncertainty; • Avian influenza planning (H5N1) used to confront 2009A(H1N1). • Foresight: • Global surveillance, genetic fingerprinting, mutations • Precaution: • International plan coordinated by WHO starting in 2005; • National plans; • Stockpiling antiviral medications; • Vaccination prioritization; • Preparation for mass fatalities (handout); • Border controls (“super-spreaders” – SARS lesson).
Pandemic Influenza Planning (PIP) • Protect the Downside: • Limiting, not avoiding, damage: • Primary effects (limiting mortality and morbidity); • Secondary effects (protecting the health care sector from collapse or serious impairment); • Tertiary effects (key business sectors, e.g., financial, need plans to avoid impacts on money and credit flows); • Fourth-order effects: provision of necessities to families. • Dealing with uncertainties: • Geographical spread through migratory birds; • Will observed severity (very high mortality) continue? (H5N1 is a type of “highly pathogenic avian influenza”); • Mutation and recombination: Will H5N1 acquire the capacity for human-to-human transmission?.
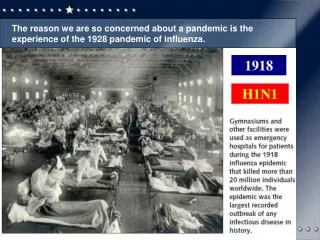
2009A (H1N1): Pandemic or not? • First outbreak, Mexico, April: This looks ominous, it’s selectively targeting healthy young adults (1918!); • (Seasonal flu is high risk for infants and elderly); • Our Winnipeg lab receives samples for gene testing; • Geographical spread versus severity (severity and ease of transmission are a trade-off for a virus; • The WHO rating scale and early difficulties; • Phase 4, human-to-human transmission • Phases 5 and 6, geographical extent [6: pandemic]; • WHO concedes that severity should be incorporated • CDC, travel advisories, criticism; • Summer: northern native communities in Canada (in 1918, the flu decimated some native communities); • July: pregnant women at elevated risk; September: Children 5-18 are at highest risk for severity.
A plague of uncertainties • Is the 2009A even worth worrying about? • Does Tamiflu really do any good? • If everybody uses Tamiflu (UK strategy), will this cause resistance and make it completely useless? • Which sub-population(s) are at highest risk? What about – especially – pregnant women? • Will a vaccine work, and can it be produced in time? • Will there be serious side-effects from the vaccine? • Should everyone be vaccinated? • Should there be priority schemes for vaccines? Can health workers refuse vaccination? • Are our hospitals ready to deal with a lot of patients with severe respiratory effects?
Uncertainty is inevitable in risk terms • Risk versus Uncertainty: • The famous distinction by Frank Knight (1921): • Uncertainty means you can’t assign a probability to a possible event; • Risk is “measurable uncertainty” (some probability can be estimated): But how confident are you about the measure? • The Uncertainty within Risk: • This has to do with level of confidence (per earlier discussion); • Numerical probability always comes with confidence interval; at 95% CI you are 95% sure that the probability range is neither higher nor lower than estimated • Example (donated blood risk for HIV): 1 in 8 million donations; range of uncertainty, 1 in 3.5 million to 1 in 20 million
The flu debates are useful! • The “objective basis” of many of these uncertainties is the cunning variation and variability of the virus itself; • Learning to manage the uncertainties that come with influenza risks is valuable for all risk management challenges: • Foresight: This is an exercise in “educated guesswork,” and of course we can get it wrong, but there are also consequences of doing nothing and just hoping for the best; • Precaution: This costs money, and we risk wasting it if we’re later proved wrong, but the consequences of not taking proper precautions can be catastrophic (see Katrina) • Protecting the Downside: To be prudent, set the expenditure on precautionary action at a level that gives some protection from the worst of the large losses we could incur if the consequences turn out to be especially severe.
Thank You! For more information or to answer questions you may have regarding this presentation, please feel free to contact Queen's Executive Development Centre: Phone: 1.888.393.2338 (1.613.533.2371) E-mail: execdev@business.queensu.ca You can also send us a request through our alumni Web site: www.queensbyyourside.ca or www.qbys.ca (accessible after the program)