Download
1 / 34
360 likes | 539 Views
Alloantibodies causing Hemolytic Disease of the Newborn and Fetus. Nancy Benitez, BS, MHS (ASCP)SBB CM Reference Laboratory Director. June 6, 2013. Case Saturday Night (SN).

E N D
Alloantibodies causing Hemolytic Disease of the Newborn and Fetus. Nancy Benitez, BS, MHS (ASCP)SBBCM Reference Laboratory Director June 6, 2013
Case Saturday Night (SN) The referring hospital transfusion service does not have any previous history on this patient as samples were received from the outpatient clinic. 32 years old Caucasian Female. Second Pregnancy
SN..cont… They reported that the antibody screen was positive with all cells tested, but due to the limited resources no further testing was performed. Samples were sent to our IRL lab for antibody Identification.
Objectives • Review the required serological techniques to determine the antibody specificity and clinical significance of alloantibodies causing Hemolytic disease of the fetus and Newborn. (HDFN) • Review the critical role that the Reference laboratory plays in the procurement of uncommon blood to transfuse the newborn. • Discuss the importance of the cooperation between patient, attending physician and the laboratory when alloantibodies are detected in the mother.
ABO-Rh DAT Screen (Liss and PEG) Panel Patient antigen testing. Routine Protocol- First Time Patients
SN Screen Liss Screen PEG Screen
Problems to resolve • Panel reacting with all cells tested. • Reactions with different strengths. • What do you think we should do next.
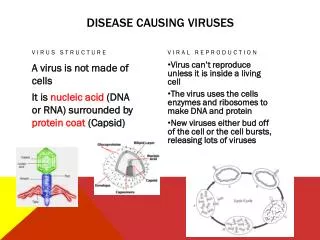
Why Patient follow up…… • Maternal IgGantibodies (anti-c, E) could be directed against the antigen(s) present on the fetal red blood cells. • IgG antibodies cross the placenta to coat fetal antigens, cause decreased red blood cell survival and produce anemia and HDNF. • Prevention for future pregnancies.
Case Saturday Night Baby (SNB) One of our local transfusion facilities requested testing for a baby sample with a possible Hemolytic Disease of the Newborn and Fetus. Mother’s records were immediately retrieve from the computer system
Case Saturday Night Baby (SNB) • The hospital also confirmed that the mother has a history of anti-c, -E. • RBCs fresh as possible, preferably <5 days old. • CMV and Hemoglobin S negative • Irradiated • Requested O Neg, c, E negative (extremely difficult combination)
Laboratory Hospital Findings- Baby • Positive Direct Antiglobulin Test • ABO-Rh: O Neg • Anemia • Hyperbilirubinemia • Reticulocytosis (6 to 40%) • Abnormal Smear
Where could we find blood • Where and how will we find a unit of blood that is Rh(D) negative and also c negative, as most of the units are dce/dce. • Blood of this type was not available in the lab
The Rh complex • The D antigen always travel with the C, c and E or e • Antigens cannot be separated
Baby’s Rh Haplotype Baby is dce / dCe Heterozygous for the Cc Antigen
Baby SN….Final outcome….. • Baby’s total serum bilirubin level was at 16 mg/dL and did not increase after phototherapy. • The Newborn was almost a Full-term an exchange transfusion was not necessary. • Baby was not severely affected because he was heterozygous for the c antigen.
Be ready…… • Think ahead, plan ahead, prepare ahead and work ahead. • Communication among the medical team and blood provider is crucial to prevent additional complications.
References Issitt PD, Anstee DJ. Applied Blood Group Serology. Montgomery Scientific Publications; Durham, NC; 1998. AABB Technical Manual, 17th edition. Mollison, PL; Engelfriet CP and Contreras M (1997). Blood Transfusion in Clinical Medicine (10th ed.). Oxford, UK: Blackwell Science.