Download
1 / 111
1.12k likes | 1.62k Views
Parathyroid and Adrenal Glands, Endocrine Pancreas. Normal Parathyroid Gland. Parenchyma consists of chief cells that secrete parathyroid hormone (parathormone, PTH) under the influence of decreasing serum calcium

E N D
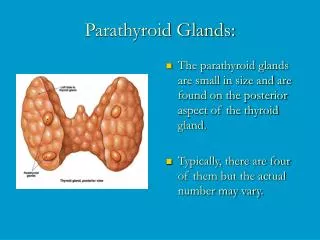
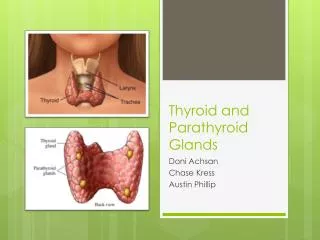
Normal Parathyroid Gland • Parenchyma consists of chief cells that secrete parathyroid hormone (parathormone, PTH) under the influence of decreasing serum calcium • There are also variable numbers of oxyphil cells in small nodules which have pink cytoplasm
Parathyroid Glands • Normal number 4 (but can be 2 or 6) • Normal combined weight 120 mg • Normal maximum dimension 6mm • Derived from epithelium and 3rd and 4th branchial clefts
Actions of Parathormone PTH • Kidney: • a.increased Ca resorbtion by tubule • b.decreased phosphate resorption • c. stimulate 1,25-OH2D3 synthesis by the kidney, thus promoting Ca absorption from the gut • Bone: increased calcium and phosphate resorption by osteoclasts • Bowel: increased calcium and phosphate absorbtion by enterocytes Net effect: raises serum calcium, lowers serum phosphate
Normal mineral metabolism Ca2+ reabsorption PO43– excretion Ca2+ Kidneys PTH Vitamin D Normal Ca2+ Parathyroidglands Ca2+ PO43– Bone Release Brown EM. In: The Parathyroids – Basic and Clinical Concepts 2nd ed. 2001. Bilezikian JP et al. (eds) PTH, parathyroid hormone
Causes and Types of Hyperparathyroidism • Primary: found in 1:1000 adults. Usually female, 30+. Adenoma 70%, hyperplasia 30% • Secondary: less common. Chronic renal disease, Vit D deficiency, malabsorbtion, ectopic hormone production • Tertiary: rare. Autonomous adenoma developing in secondary hyperplasia
Features of Hyperparathyroidism • Malaise, constipation, muscle weakness, neuropsychiatric disorders • renal colic due to stones (60%) • bone pain due to generalised Ca loss • peptic ulcer (10%) • acute pancreatitis • nephrocalcinosis • raised serum calcium and PTH • raised urinary PO4 and serum alk phos • raised urinary hydroxyproline
Osteitis Fibrosa Cystica • Classic localised bone lesion of hyperparathyroidism. Bone is lysed by osteoclasts driven by elevated PTH. Marrow replace by highly vascularised fibrous tissue. Stress on weakened bone causes haemorrhage and cyst formation. • Old term for this lesion was “brown tumour”. Colour due to massive haemosiderin deposition • Typically found in jaw and long bones and may cause pathological fractures • Can be distinguished from other giant cell tumours of bone by estimation of serum Ca.
Causes and features of Hypoparathyroidism • Injury or removal: surgery, birth trauma, autoimmune destruction • Receptor defect: X-linked dominant receptor deficiency- so-called pseudohypoparathyroidism • Clinical features: tetany, low Ca, high PO4, low urine PO4
Pathogenesis of diseases of the Adrenal Glands and Endocrine Pancreas
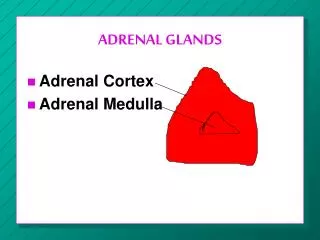
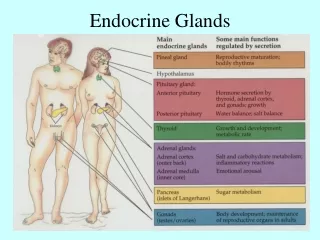
Adrenal Glands • Cortex: zona glomerulosa, zona fasicularis, zona reticulosa • Aldosterone: re-absorbtion of NA, loss of K • Glucocorticoids: gluconeogenesis, anti-inflammatory • Androgens: anabolic, virilizing • Medulla: sympathetic nerve cells, produce adrenaline and noradrenaline
Causes of Cushing Syndrome (hypersecretion of glucocorticoids) • Iatrogenic: corticosteroid therapy • Pituitary origin: basophilic adenoma or hypothalamic dysfunction • Adrenal origin: cortical adenoma, carcinoma, hyperplasia • Ectopic ACTH production: small cell carcinoma of lung, islet cell tumours, other neoplasms
Manifestations of Cushing Syndrome • Psychosis • Polycythaemia • Moon face • Buffalo hump • Striae • Truncal obesity • Muscle Wasting • Acne, hirsutism, hypertension, hyperglycaemia, osteoporosis • Amenorrhoea , impotence
Hypocorticoadrenalism (acute) • Increased demand for steroids in the face of chronic insufficiency (e.g. Addison’s) • Bilateral adrenal necrosis due to viremia (e.g.herpes), Gram- septicemia, and/or DIC. Necrosis often haemorrhagic- typified by the Waterhouse-Friederichsen syndrome • Features of acute insufficiency: profound hypotension (shock), vomiting, dehydration, low serum Na, high K
Hypocorticoadrenalism (chronic) • Usually referred to as Addison’s disease, and caused by either: • Autoimmune destruction of adrenal cortex in which there is a strong association with other autoimmune diseases e.g. PA, Type 1 diabetes, Hashimoto thyroiditis or • Metastatic tuberculosis of the adrenals
Addison’s Disease • Clinical manifestations: extreme muscle weakness,hypotension, hypoglycaemia, pigmentation buccal mucosa • Biochemical manifestations: low serum sodium, glucose and cortisol high serum potassium and ACTH high urinary sodium
Tumours of Adrenal Cortex • Adenoma: common, benign, and mostly non-functional. Found at autopsy in 2% of population. More frequent in hypertensives (20%), women > 80 (30%), obese diabetics (30%) • Carcinoma: rare, functional in 50%. May cause Cushing’s syndrome (50%), virilization (30%), feminisation (12%), Conn’s syndrome (4%)
Conn’s Syndrome (hyper-mineraloadrenocorticism) • Clinical Features: hypertension due to sodium retention muscle paralysis due to hypokalemia polyuria and polydipsia susceptibility to pyelonephritis low plasma rennin
Conn’s Syndrome: pathogenesis • Cortical adenoma (aldosteronoma) 90% • Nodular cortical hyperplasia 10% • Adrenocortical carcinoma- very rare
Tumours of Adrenal Medulla: neuroblastoma • < 3 years, M=F • highly malignant PNET that commonly presents with mets e.g. skull (Hutchinson) or liver (Pepper) • sporadic and familial forms • N-myc amplified in up to 80% of cases have deletion of distal short arm of Ch1 • Early lesions with ganglion cells have much better prognosis (94% 2 yr survival)
Tumours of Adrenal Medulla: phaeochromocytoma • a paraganglioma, 30-50 yrs, M=F • 10% bilateral, 10% malignant, 10% extra-adrenal • secretes noradrenaline producing hypertension, tachycardia, glycosuria, pallor and sweating • elevated urinary VMA
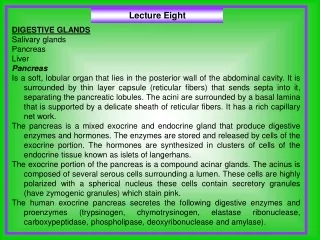
Diseases of the Endocrine Pancreas[slides 45-103- for personal revision]
Diabetes Mellitus • Definition A chronic systemic disease characterised by absolute or relative lack of insulin and abnormalities of structure and function of blood vessels
Diabetes Mellitus • Disorder of Metabolism- carbohydrate, protein and fat • Characterised by hyperglycaemia • Clinically; polyuria, polydipsia, polyphagia
Diabetes Mellitus • Diabetes mellitus (sweet urine) • 3% world population, 100 million people • Incidence increasing alarmingly (40% in the past decade, more in future, 259m by 2025) • Most common non-communicable disease • High morbidity and mortality • Shortens life span by 15 years • Leading cause of blindness and kidney disease
Normal Pancreatic Islet: ß α ß cells (Insulin)αcells (Glucagon) δ cells (Somatostatin) pp Cells (polypep)