Download
1 / 48
480 likes | 665 Views
Adrenal and Parathyroid Disease. J.B. Handler, M.D. University of New England Physician Assistant Program. DHEA- dehydroepiandosterone ACTH- adrenocorticotropic hormone RA- rheumatoid arthritis SLE- systemic lupus erythematosis DM- diabetes mellitus VMA- vanillylmandelic acid

E N D
Adrenal and Parathyroid Disease J.B. Handler, M.D. University of New England Physician Assistant Program
DHEA- dehydroepiandosterone ACTH- adrenocorticotropic hormone RA- rheumatoid arthritis SLE- systemic lupus erythematosis DM- diabetes mellitus VMA- vanillylmandelic acid PGA- polyglandular autoimmune MEN- multiple endocrine neoplasia RIA- radioimmune assay cAMP- cyclic AMP PUD- peptic ulcer disease NS- normal saline RL- Ringer’s lactate DDx- differential diagnosis DM- diabetes mellitus Abbreviations
Adrenal Cortex • Aldosterone secretion localized to outer layer of adrenal cortex-regulated by renin secretion by kidneys; mineralocorticoid effects on renal tubules- Na, K, etc. RegulationRAAS. • Cortisol: Major glucocorticoid secreted by middle and inner adrenal cortex; multitude of effects; necessary for life. Secretion regulated by ACTH release from pituitary. • Androgens>estrogens: Inner adrenal cortex; testosterone, androstenedione, DHEA, estradiol. Regulation complex ACTH and other factors.
Cortisol (Hydrocortisone) • Diurnal pattern of secretion by adrenal carbohydrate metabolism and more. • Inhibits insulin secretion; increases hepatic gluconeogenesis, s protein stores(synthesis,catabolism). Note: physiologic effects vs excess (see below). • Dampens defense mechanisms • Inhibits production or action of many mediators of inflammation • Required for production of Angiotensin II • Lowers serum calcium (kidney and GI) • Necessary for normal bodily function
Cortisol • Secreted in response to stress, trauma, infection, and major surgery. Plays a major role in supporting normal circulatory function and hemodynamic stability in response to a variety of stresses. • “The permissive hormone”. • Has weak mineralocorticoid effects. • Normal daily secretion 15-25mgs.
Cushings Syndrome/Disease • Clinical syndrome/disease resulting from excessive systemic corticosteroids; multiple etiologies. • Sources: • Endogenous over production: tumors secreting cortisol or ACTH (Cushings Disease). • Exogenous glucocorticoidadministration(drugs)- superphysiologic doses over prolonged time. Most common cause of Cushings syndrome.
Endogenous Glucorticoid Excess • Cushing’s syndrome: • Adrenal tumor (32%) -adenoma or carcinoma secreting excessive cortisol. ACTH suppressed (feedback loop)remaining normal adrenal tissue inactive. • Non-pituitary neoplasms (lung Ca) producing excessive, ectopic ACTH (10%). • Unidentifiable source of ectopic ACTH (15%) • Cushings Disease (43%): Pituitary adenoma secreting excessive ACTH. • Above etiologies are rare.
Signs and Symptoms • Central obesity: “moon facies”, abdominal protuberance, “buffalo hump”, supraclavicular fat. Catabolic effects: thin skin with easy bruising & striae, thin extremities, muscle wasting. Other: acne, hirsutism; impaired healing. • Glucose intolerance/DM, hypertension, oligomenorrhea, amenorrhea, impotence. • Weakness, headaches, increased thirst & polyuria (high glucose). • Osteopenia and osteoprosis (bone protein).
Cushing’s Syndrome/Disease Images.google.com
Laboratory Findings and Testing • Hyperglycemia, glycosuria, leukocytosis. • Elevated Cortisol levels with loss of diurnal pattern. • In excess ACTH states, increased mineralocorticoid can lead to hypokalemia. • Dexamethasone suppression test: 1 mg given at 11 PM. AM cortisol should be low (<5ug/dL). • 24 hour urine free cortisol/creatinine (>95ug cortisol/gram creatinine confirms hypercorticolism). • ACTH level: Adrenal vs other etiologies • MRI of head, CT of chest and abdomen (lungs, pancreas, adrenals, thymus)
Complications if Untreated • Significant morbidity from diabetes, hypertension, susceptibility to infections, compression and pathologic fractures, femoral neck aseptic necrosis. • Treatment: Transphenoidal resection of pituitary adenoma; laparoscopic resection of adrenal tumors. Good prognosis if resection is complete. • Post-op Rx with cortisol often needed. • Ketoconazole and metyrapone- metastatic adrenal Ca.
Exogenous Glucorticoid Excess • Most common scenario is prolonged administration of synthetic, exogenous glucocorticoids in supraphysiologic doses (2-40x normal). This leads to chronic suppression of ACTHand the adrenals and clinical picture of hypercorticolism. • Most common cause of Cushings syndrome • Significant associated morbidity over time, similar to endogenous excess.
Exogenous Glucorticoid Excess • Development dependent on the dose, duration, and timing of administration • Many synthetic glucocorticoids available • Most popular is prednisone (4x cortisol potency) • Chronic suppression of adrenal gland important if/when glucocorticoids are discontinuedmust taper (see below). • Examples: Chronic severe asthma, post transplantation, polymyalgia, SLE, cancer chemotherapy, sarcoidosis, etc.
Case 1 • A 42 y/o man is brought to the ED c/o weakness, dizziness and abd. pain. He developed “flu” like symptoms 24 hrs ago with cough, aching and temp. No major med problems but has been on a 1x daily drug x yrs for uncertain reasons; does not recall the name. • PE- ill appearing male, moaning; T=101, P-110, BP- 80/50. Lungs- clear, heart- regular tach without murmur; abd- soft, non-tender to deep palpation. • Differential diagnosis? Thoughts?
Adrenal Insufficiency • Broad spectrum of signs and symptoms characteristic of glucocorticoid deficiency. • Signs and symptoms are non-specific and involve more than one organ system. Diagnosis may be difficult- must have index of suspicion; important to include in DDx of patients with fatigue, weakness and hypotension. • Acute and chronic presentations.
Patients at Risk for AI • Taking exogenous corticosteroids with suppression of the hypothalamic-pituitary-adrenal axis.Patient at risk for AI if: • Requirement for cortisol increases: stress, trauma, infection, MI, surgery, etc. • Glucocorticoid (e.g. prednisone) is tapered too rapidly for suppressed adrenal to resume normal secretion chronic or acute picture. • Autoimmune adrenal disease: Addison’s disease.
Chronic Adrenal Insufficiency • Addison’s Disease- Uncommon disease; autoimmune destruction of the adrenal cortex that can develop over time resulting in chronic deficiency of cortisol, aldosterone and adrenal androgens. • May be a component of PGA syndromes involving multiple glands (Parathyroid, Thyroid, Pancreas) • Bilateral adrenal hemorrhage (anticoagulant’s, trauma); pituitary destruction with ACTH deficiency.
Symptoms and Signs • Weakness, fatigue, wt. loss, myalgias, arthralgias, N&V, diarrhea, abdominal pain, anxiety, irritability. • Must have index of suspicion as sx are non-specific and often present with other illnesses/diseases. • Low BP, orthostasis, hyperpigmentation of skin, including knuckles, palmar creases, elbows, knees, nipples and nailbeds; reduction of axillary and pubic hair.
Chronic Adrenal Insufficiency Images.google.com
Investigative Findings • LAB: Neutropenia, lymphocytosis, eosinophilia; low AM cortisol level (<5ug/dL); hyponatremia, hyperkalemia. • Diagnostics: Abdominal CT (small non-calcified adrenals): Addison’s)
Diagnostic Testing: Acute or Chronic AI • Cosyntropin (synthetic ACTH) stimulation test: cosyntropin 250 ug given IV/IM- serum cortisol obtained in 30-60 minutes; normal response is rise in serum cortisol to at least 20 ug/dL. Provides measure of adrenal reserve. • If pt is on Hydrocortisone replacement Rx dose must be held at least 8 hours before the test. Use of synthetic glucocorticoids (dexamethasone) do not interfere with testing.
Treatment: Chronic Adrenal Insufficiency • Glucocorticoid replacement following diurnal pattern: hydrocortisone 15-20 mg in A.M, 5-10 mg in P.M. • Mineralocorticoid replacement if necessary with fludrocortisone .05-.2 mg/daily. • Must increase (8-10x) maintainence cortisol dose during periods of stress (infection, trauma, surgery, MI) to avoid acute adrenal insufficiency/crisis.
Acute Adrenal Insufficiency • Life threatening medical emergency. • Most often seen in patients with suppressed adrenal gland who develop need (medical stress) for additional cortisol (infection, surgery, MI, etc.). • Suppressed gland from exogenous glucocorticoids is most common scenario but also occurs in patients with Addison’s. • Must have high index of suspicion in all patients taking exogenous glucocorticoids chronically.
Acute Adrenal Insufficiency/Crises • May be precipitated by rapid or abrupt withdrawal of corticosteroids in a patient previously taking these drugs for prolonged periods. Must taper steroid dose before they are discontinued to allow adrenal pituitary axis to recover (may take several weeks or more). • Post adrenal or pituitary surgery.
Signs, Symptoms and LAB • Headache, nausea, vomiting, confusion, abd. pain, diarrhea, temp. (>40), severe hypotension, cyanosis, dehydration and hemodynamic collapse. • Consider acute AI in patient with hypotension/shock unresponsive to IV fluids and pressors. If diagnosis is suspected, draw blood for cortisol level (don’t wait for results) and Rx with IV hydrocortisone (see below).
Signs, Symptoms and LAB • Labs: Hypoglycemia, eosinophilia, hyponatremia, hyperkalemia, cortisol. • High ACTH levels if Addison’s present. Cosyntropin stimulation test (above)- confirms diagnosis.
Treatment • Rapid infusion of isotonic fluds (NS, RL). • IV Hydrocortisone in pharmacologic doses (100-300mgs) repeated q6hrs until hemodynamically stable. Alternative is continuous IV infusion of 10mg/hr. • Treat underlying physiologic stress. • Eval for etiology if not yet known. • Oral hydrocortisone once stable.
Case 1 • Initial treatment: IV- NS 500 cc over 10” followed by 250 cc/hr- no change in BP. Dopamine in increasing dose via IV infusion- only slight increase in BP. • Hydrocortisone 100 mg IV push- BP began to rise within minutes; gradual improvement over next 6 hours.
Case 1 • Labs: Na 130 meq/L, K-5.1 meq/L, glucose-80 mg/dL; WBC- 4500 x 106 with lymphocytosis. • Diagnosis? • Subsequent info: wife brings in his med (prescribed in Canada): “deltasone” 5 mg/d. • Further diagnostic testing?
Pheochromocytoma • A rare cause of secondary hypertension. • Tumor of the adrenal medulla (occasionally elsewhere) releasing excessive amounts of norepinephrine/epinephrine into the circulation.
Pheochromocytoma • Hypertension (sustained or paroxysmal) with paroxysms of symptoms including severe headaches, sweating and palpitations. • Dx: 24 hr urine for catecholamines & metanephrines
Evaluation and Treatment • Abdominal CT/MRI, nuclear imaging • Complications: hypertensive crisis, stroke or intracerebral bleed, cardiomyopathy. • Laparoscopic removal of the tumor is the treatment of choice. Preoperative administration of alpha blocking drugs (phenoxybenzamine) and beta blockers can reduce perioperative complications.
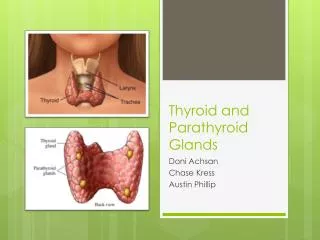
Parathyroid and Ca Homeostasis • Parathyroid Hormone (PTH)- major effects: • Helps maintain calcium homeostasis in the body. Increases osteoclastic activity in bone resulting in delivery of Ca and PO4 into circulation. • Increases renal tubular reabsorption of Ca. • Increases PO4 excretion in urine. • Stimulates synthesis of 1,25 dihydroxycholecalciferol by the kidney (Vit. D metabolite) resulting in increased absorption of Ca from GI tract.
Parathyroid and Ca Homeostasis • Regulates and maintains normal levels of serum ionized calcium. Urinary cyclic AMP excretion is sensitive index of PTH activity. • Long-term actions: Stimulates osteoclasts and osteoblasts (bone remodeling). Usually osteoclastic activity predominates to maintain Ca levels. • Pharmacologic actions of intermittent synthetic PTH injection are paradoxical (to be discussed with Osteoporosis treatment).
Calcium Metabolism • 1% total body calcium is in solution.50% ionized, 40% protein bound, 10% complexed with anions (citrate,etc.). • Normal serum Ca is 9-10.3 mg/dL. • Ionized Ca is 4.7-5.3 mg/dL. • Important to measure serum albumin and “correct” total Ca if albumin is low: • “Corrected” serum Ca= serum Ca mg/dL + (0.8 x [4.0-Albumin g/dL])
Hypoparathyroidism • Hallmark is low ionized Ca. Most common scenario is post-thyroidectomy or post removal of parathyroid adenoma(where other parathyroid glands are suppressed). Uncommon. • Rarely autoimmune associated with PGA. • May develop with chronic magnesium deficiency which can impair PTH release; reversible.
Signs and Symptoms • Dependent on how long disease is present. • Acute: Muscle cramps, irritability, carpopedal spasm, tetany, seizures, paresthesias of hands and feet. • Chronic: Lethargy, personality changes, cognitive function, cataracts. • Chvostek’s sign, Trousseaus’s sign. • Dry, thin nails, hyperactive reflexes.
Lab and Diagnostics • Low serum total and ionized Ca, elevated PO4, normal alkaline phosphatase, low urine Ca. PTH levels. Important to check Mg level and Rx if low. • ECG: prolonged Q-T interval and arrhythmias.
Differential Dx of Low Ca • Hypoparathyroidism • Malabsorbtion • Vitamin D deficiency • Hypomagnesemia
Treatment • Acute: IV Calcium gluconate until tetany and other acute symptoms resolve. • Chronic: Oral Calcium 1-2 grams PO daily. • Active metabolite of Vitamin D: 1,25-dihydroxycholecalciferol (calcitriol). • Magnesium supplement as needed. • Goal is to maintain serum Ca in low normal range.
Hyperparathyroidism • Hypersecretion of PTH, most often a parathyroid adenoma (.1% incidence). • Hallmark is elevation of serum total & ionized Ca. • Increased excretion of Ca and PO4 by the kidney (overwhelms tubular Ca absorptive capacity) hypercalciuria. • Chronic cortical bone resorption. If severe: Diffuse demineralization, osteopenia, osteoporosis pathologic fractures.
Osteoporosis Images.google.com
Signs and Symptoms • Often discovered as anincidental lab finding in asymptomatic patientCa. • If symptoms: “moans, groans, stones, bones”. • Skeletal: Loss of cortical bone with bone pain and arthralgias. • GU: Hypercalcemia/hypercalciuria results in nephrogenic DI (sensitivity to ADH), with polyuria and polydipsea. Calcium stones, nephrosclerosis and renal failure can occur. • If Ca : anorexia, lethargy, fatigue, weakness; altered MS; nausea, constipation, pancreatitis; BP.
Lab and Diagnostics • Serum Ca > 10.5 mg/dL (when corrected for albumin, if low). • Increased ionized calcium (>5.4 mg/dL). • PO4 often low (enhanced renal excretion). • Alkaline Phosphatase elevated in the presence of bone disease. • PTH assay via RIA, urine cAMP. • Imaging usually unable to define parathyroids unless there is a large adenoma (MRI, Tc99). • Surgery often performed with unguided neck exploration if adenoma likely.
Complications: Severe Disease • Pathologic fractures, especially in women. • Urinary stones, obstruction, UTI’s. • If Ca rises rapidly- CNS changes, renal failure. • PUD and pancreatitis from high Ca levels.
Differential Diagnosis (Ca) • Hypercalcemia of malignancy- tumor metastasis to bones (breast, lung, pancreas, kidney) leading to bony erosion. These tumors may also secrete PTH related proteins leading to bony resorption & hypercalcemia. • Multiple myeloma- bone marrow cancer. • Milk-alkali-vitamin D syndrome. • Sarcoidosis • Artifact- lab error
Treatment • Acute Rx of Ca:NS + furosemide; IV bisphosphonates (inhibit bone resorption). • Parathyroidectomy indications:Symptomatic patients; presence of bone disease or kidney stones.Asymptomatic patients- Hypercalcemia with significant hypercalciuria; cortical bone density 2 SD below normal, age <50, Ca>1.0 mg/dL above upper limit of normal, pregnancy (2nd trimester).
Treatment • Complications of surgery: rapid drop on PTH levels resulting in acute hypocalcemia post-op. Calcium supplements until remaining parathyroids resume function.