Download
1 / 29
310 likes | 453 Views
Multiple sclerosis. Pathology. Key principles. Myelin function The differences between CNS and PNS Myelin Primary Demyelinating disease classification

E N D
Multiple sclerosis Pathology
Key principles • Myelin function • The differences between CNS and PNS Myelin • Primary Demyelinating disease classification • Multiple sclereosis: definition, epidemiology, pathogenesis and clinicopathological features; with special emphasis on CSF analysis findings, morphology and distribution of MS plaques.
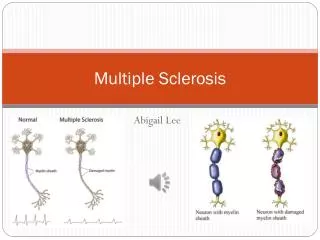
Myelin • Myelin consists of multiple layers of the specialized plasma membrane of oligodendrocytes (in the CNS), with most of the cytoplasm excluded • Although myelinated axons are present in all areas of the brain, they are the dominant component in the white matter; therefore, most diseases of myelin are primarily white matter disorders. What is the function of myelin?
Myelin • An oligodendrocyte extends processes toward many different axons and wraps a segment of roughly a few hundred microns of axon • Each of these segments is called an internode, and the gaps between internodes are known as nodes of Ranvier
MyelinThe differences between CNS and PNS • The myelin in peripheral nerves is similar to the myelin in the CNS but: • peripheral myelin is made by Schwann cells, not oligodendrocytes • each cell in the peripheral nerve contributes to only one internode, while in the CNS, many internodes comes from a single oligodendrocyte • the specialized proteins and lipids are also different • Most diseases of CNS myelin do not significantly involve the peripheral nerves, and vice versa
The natural history of demyelinating diseases is determined, in part, by the limited capacity of the CNS to regenerate normal myelin and by the degree of secondary damage to axons that occurs as the disease runs its course What is “natural history of a disease”?
Primary Demyelinating disease general classification • Two broad groups: • Demyelinating diseases of the CNS: • acquired conditions characterized by preferential damage to previously normal myelin • commonly result from immune-mediated injury • also viral infection of oligodendrocytes as in progressive multifocal leukoencephalopathy • drugs and other toxic agents. • Dysmyelinating diseases of the CNS: • myelin is not formed properly or has abnormal turnover kinetics • associated with mutations affecting the proteins required for formation of normal myelin or in mutations that affect the synthesis or degradation of myelin lipids • the other general term for these diseases is leukodystrophy.
Multiple sclerosis • MS is an autoimmune demyelinating disorder characterized by distinct episodes of neurologic deficits, separated in time, attributable to white matter lesions that are separated in space • The most common demyelinating disorders (prevalence of 1 per 1000 persons in most of the United States and Europe)
Multiple sclerosis • The disease becomes clinically apparent at any age, although onset in childhood or after age 50 years is relatively rare • Women are affected twice as often as men • In most individuals with MS the illness shows relapsing and remitting episodes of neurologic deficits The frequency of relapses tends to decrease during the course of the illness, but there is a steady neurologic deterioration in a subset of patients
Multiple sclerosisPathogenesis • Like other autoimmune diseases, MS is believed to be caused by a combination of environmental and genetic factors that result in a loss of tolerance to self proteins
Multiple sclerosisPathogenesis • The risk of developing MS is 15-fold higher when the disease is present in a first-degree relative • The concordance rate for monozygotic twins is approximately 25%, with a much lower rate for dizygotic twins • A significant fraction of the genetic risk for MS is attributable to HLA-DR variants, the DR2 allele being the one that most significantly increases the risk for developing MS
Multiple sclerosisPathogenesis • Experimental allergic encephalomyelitis is an animal model of MS in which demyelination and inflammation occur after immunization with myelin, myelin proteins, or certain peptides from myelin proteins • In this model, the lesions are caused by a T cell-mediated delayed type hypersensitivity reaction to myelin proteins, and the same immune mechanism is thought to be central to the pathogenesis of MS
Multiple sclerosisPathogenesis • While MS is characterized by the presence of demyelination out of proportion to axonal loss, some injury to axons does occur • Toxic effects of lymphocytes, macrophages, and their secreted molecules have been implicated in initiating the process of axonal injury, sometimes even leading to neuronal death.
Multiple sclerosisMorphology • MS is a white matter disease • Affected areas show multiple, well-circumscribed, slightly depressed, glassy, gray-tan, irregularly shaped lesions, termed plaques • They occur beside ventricles and they are frequent in the optic nerves and chiasm, brain stem, ascending and descending fiber tracts, cerebellum and spinal cord
Multiple sclerosisMorphology • The lesions have sharply defined borders at the microscopic level
Multiple sclerosisMorphology • In an active plaque there is evidence of ongoing myelin breakdown with abundant macrophages containing myelin debris • Lymphocytes and monocytes are present, mostly as perivascular cuffs • Axons are relatively preserved, although they may be reduced in number
Multiple sclerosisMorphology • When plaques become quiescent (inactive plaques), the inflammation mostly disappears, leaving behind little to no myelin • Instead, astrocytic proliferation and gliosis are prominent
Multiple sclerosis Clinical Features • The course of MS is variable. MS lesions can occur anywhere in the CNS may induce a wide range of clinical manifestations • Commonly there are multiple episodes of new symptoms (relapses) followed by episodes of recovery (remissions); typically, the recovery is not complete • The consequence of this pattern of relapsing-remitting disease is the gradual, often stepwise, accumulation of increasing neurologic deficits
Multiple sclerosis Clinical Features • certain patterns of neurologic symptoms and signs are commonly observed: • Unilateral visual impairment occurring over the course of a few days is a frequent initial manifestation of MS (due to involvement of the optic nerve “optic neuritis”) • When this occurs as the first event, only a minority (10% to 50%) go on to develop full-blown MS • Involvement of the brain stem produces cranial nerve signs and ataxia, and can disrupt conjugate eye movements • Spinal cord lesions give rise to motor and sensory impairment of trunk and limbs, spasticity, and difficulties with the voluntary control of bladder function
Multiple sclerosis Clinical Features • Changes in cognitive function can be present, but are often much milder than the other findings • In any individual patient it is hard to predict when the next relapse will occur; most current treatments aim at decreasing the rate and severity of relapses rather than recovering lost function
CSF findings • It shows mildly elevated protein level with an increased proportion of γ-globulin • In one-third of cases there is moderate pleiocytosis • When the immunoglobulin is examined further, most MS patients show oligoclonal bands, representing antibodies directed against a variety of antigenic targets • These antibodies constitute a marker for disease activity
Don’t miss youtube videos on MS, many are of great quality..