Download
1 / 20
240 likes | 552 Views
Bile Peritonitis. Signalment. Tanner, 6.5 yo MC Cocker Spaniel. History. 1 week history of vomiting (yellow liquid), diarrhea, anorexia Has been seen at rDVM for 1 week with inc ALP, ALT, GGT, T-bili, dec BUN, glucose, elevated bile acids, fever, inflammatory leukogram

E N D
Signalment • Tanner, 6.5 yo MC Cocker Spaniel
History • 1 week history of vomiting (yellow liquid), diarrhea, anorexia • Has been seen at rDVM for 1 week with inc ALP, ALT, GGT, T-bili, dec BUN, glucose, elevated bile acids, fever, inflammatory leukogram • Has been treated with enrofloxacin, metronidazole, famotidine and maropitant
Physical Exam Findings • Abdomen tense and painful (1-2/4) on palpation • Obese • T: 103.2F P: 132bpm R: 24 br/min • CRT <2sec Wt 17.6kg BCS: 7/9
Clinical Pathology • CBC: marked leukocytosis (62.51K/uL RR: 4.39-11.61) characterized by a neutrophilia (51.883K/ul RR: 2.841-9.112) with a regenerative left shift (1.250K/ul bands) and monocytosis (8.126K/ul RR: 0.075-0.85). Mild microcytic, hypochromic anemia (Hct = 32.1%). Thrombocytopenia (150K/uL) with increased MPV. Mild hypoproteinemia (5.8 g/dL RR: 6.1-7.5).
Clinical Pathology • Chemistry Panel: • Markedly elevated ALP (3804 IU/L), mildly elevated ALT, GGT and T-bili, hyperphosphatemia, hypocalcemia, hypomagnesemia, hypoalbuminemia, low normal glucose, low normal BUN. Electrolytes are within normal limits.
Clinical Pathology • Resting Ammonia: Increased at 43 umol/L (RR: 3-30). • Bile Acids Tolerance: Increased resting and post-prandial levels (pre = 55.7, post = 71.5 umol/L RR: 25) • Coagulation Profile: High normal PT, prolonged PTT. D-dimers 500-1000 ng/ml. Thrombocytopenia.
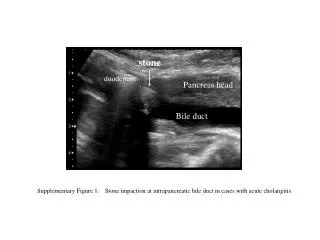
Abdominal Ultrasound • Probable hepatic cirrhosis - no evidence of portal hypertension • Biliary mucocele • Hepatic lymphomegaly - probable reactive hyperplasia • Right adrenomegaly - hyperplasia vs. neoplasia
Abdominal Fluid Analysis • Highly cellular specimen with large numbers of inflammatory cells with a pale blue to green mucinous material that is consistent with bile. Rare bilirubin crystals noted. Inflammatory cells consist of 84% slightly degenerate neutrophils and 16% activated macrophages. • Interpretation/assessment: Bile peritonitis with marked suppurative inflammation • Bilirubin: 1.5mg/dL (Serum 2.0mg/dL)
Outcome • Owners elected to euthanize based on the diagnosis of bile peritonitis • Necropsy: Microhepatica with diffuse nodules, distended gall bladder with inspissated brown-green mucoid material and rupture of the common bile duct, fibrin at the defect and diffusely throughout abdomen, bile and inflammation throughout the mesentery, thoracic lymphadenopathy