Download
1 / 43
460 likes | 730 Views
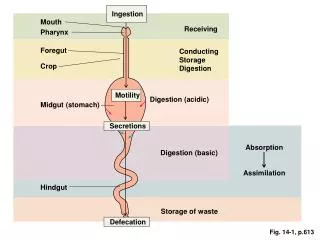
Esophageal Motility Disorders. Anatomy. Active muscular organ with a complex neuromuscular structure and integration. The sequential muscular contractions push food from above and clear acid and bile reflux from below. Specialized sphincter at each end. UES and LES. Anatomy.

E N D
Anatomy • Active muscular organ with a complex neuromuscular structure and integration. • The sequential muscular contractions push food from above and clear acid and bile reflux from below. • Specialized sphincter at each end. • UES and LES
Anatomy • UES contracts during inspiration preventing air from entering into the GI tract, while the LES maintains a steady baseline tone to prevent gastric juice from refluxing into the esophagus. • LES also contracts during periods of increased intraabdominal pressure, preventing reflux due to pressure in the abdomen. • Inner circular layer, outer longitudinal layer of muscle. (ring occlusions and shortens)=> peristalsis.
Peristalsis • Sequential, coordinated contraction wave that travels along the whole length of the esophagus, propelling intraluminal contents downstream. • Primary wave strips from proximal to distal, triggered by swallowing center, 2cm/sec. • Secondary wave induced by distension of bolus, acts to clear esophagus of retained food. • Tertiary contractions are dysfunctional and have no role.
Motility Disorders • Achalasia • Primary spastic motility disorders, including DES, nutcracker esophagus, hypertensive LES • Secondary esophageal motility disorders related to DM, scleroderma, alcohol, psychiatric disorders, etc.
Achalasia • Loss of ganglion cells from the wall of the esophagus, starting at the LES and going proximally. • Loss of inhibitory nerves at LES. • Circular muscle layer thickened at LES but microscopically cells appear normal.
Achalasia • Loss of the inhibitory nerves at the LES causes failure of the LES to completely relax, and a hypertensive LES pressure over 40mmHg in 60% of patients. • Loss of nerves along the body of esophagus causes aperistalsis, stasis, dilatation.
Achalasia • Non-peristaltic isolated contractions or low-amplitude simultaneous contractions occur. • If high-amplitude (>60mmHg) simult contractions occur it is called Vigorous Achalasia.
Achalasia • Edrophonium (acet cholesterase inhib) increases LES pressure. • Atropine reduces the LES pressure in achalasia, which is why botulinum toxin can be therapeutic (ach release inhibitor).
Spastic Motility Disorders • Diffuse fragmentation of vagal filaments, mitochondrial fragmentation results in functional imbalance between excitatory and inhibitory pathways. • When DES occurs, diffuse muscular hypertrophy as much as 2cm has been described in the distal 2/3 of the esophagus, but wall thickening is also found in asymp patients, absent in patients with typical sympt and manometric findings too.
Scleroderma Esophagus • Primary defect here is related to smooth muscle atrophy and fibrosis. • The dysmotility here an absence of peristalsis in the esoph body and an atonic LES occur. • Motility is preserved at the striated muscle part of the esophagus.
Frequency • Achalasia and DES only a small percentage of disorders of motility. • Achalasia 1 case per 100,000 per year. • Familial clustering occurs but not genetic yet. • Nutcracker esoph is most common motility disorder, but the most controversial in significance.
Mortality and Morbidity • Achalasia associated with significant progressive discomfort, severe dysphagia, malnutrition, weight loss, dehydration. Increased incidence of SCC with long standing disease. • Spastic motility disorders are associated with sympt discomfort but not the severity of dysphagia as in achalasia. • Scleroderma associated with severe acid reflux, associated complications, including strictures, Barretts, adenocarcinoma.
Race, Sex, and Age • Racial differences not established. • Affects both sexes equally. • Achalasia presents in patients 25-60 yrs, although it can affect any age group.
History • Achalasia: progressive dysphagia for both solids an liquids is a hallmark. Regurge of food in dilated esoph common especially at night. Chest pain, sensation of heartburn (fermentation). Emotional stress or rapid eating makes it worse. • Spastic disorders: Chest pain hallmark, mimics angina, may be related to transient esoph ischemia, distension. Dysphagia to solids and liquids a common symptom, especially with DES, intermittent, non-progressive. Heartburn, regurge.
History • Scleroderma: involves esoph in 75% of patients. • Two forms- PSS a progressive form that is more fulminant, early involvement with internal organs; CREST- calcinosis, Raynauds phenomena, esoph dysfunction, sclerodactyly, telangiectasia. • Severe acid reflux, regurge, dysphagia, erosive esophagitis (60%), increased incidence of cancer • Dysphagia from peptic strictures, poor peristalsis.
Physical • Results of a physical exam are usually unrevealing. • Pay attention to signs of scleroderma in proper clinical setting. • A bedside swallowing challenge can be performed with a glass of water. • Check nutrition and hydration if dysphagia reported.
Causes • Primary disorders are idiopathic in nature. • Viral • Infectious • Environmental • Genetic
Other Problems • Differential diagnosis depends on presenting symptoms. • CAD, mechanical obstructing lesions, benign or malignant should be ruled out. • Differential of achalasia includes Chagas disease secondary to Trypanosoma cruzi infection and pseudoachalasia from GE junction tumors.
Chagas Disease • Mimics achalasia. • Reduviid (kissing) bug bite. • Endemic in SA, CA. • Septicemia first, then chronic stage ensues. • Widespread ganglion destruction throughout the body involving heart, gut, GI tract, urinary tract, respiratory tract. • Symptoms take years to develop. • Treatment: disrupt LES like in achalasia.
Pseudoachalasia • Term used to describe clinical picture of GE junction obstruction. • Present in 5% of patients with clinical and manometric diagnosis of achalasia.
Pseudoachalasia • Clinical presentation is more likely to occur with rapidly progressive disease, older age of onset, profound weight loss. • Workup includes upper endoscopy, biopsies should be obtained with any suspicion of malignant process. If suspicious lesion found, image with CT, MRI, EUS if indicated. • In 50% of patients the diagnosis is adenocarcinoma of GE junction.
Diffuse Esophageal Spasm • DES and achalasia can be confused. Manometric criteria require that normal esophageal peristalsis be present intermittently for DES. • LES relaxation, which is incomplete in achalasia, should be normal in DES.
Workup • CXR: Dilated esophagus, looks sigmoid like, air fliud level, wide mediastinum, absence of gastric air bubble. • Esophagram: In achalasia, dilated, A-F level, tapered LES, bird’s beak appearance. Diverticula above LES, hiatal hernia. In DES corkscrew or rosary bead esophagus. In scleroderma, slightly dilated esophagus, absent peristalsis, free reflux.
Manometry • Achalasia: aperistalsis of esophageal body is manometric hallmark. • DES: Normal peristalsis, simultaneous contractions in >30% water swallows, incomplete LES relaxation, increased LES pressure (>40mmHg), or repetitive, prolonged(>6sec), high-amplitude contractions (>180mmHg).
Manometry • Nutcracker: Normal patterned peristalsis with high amplitude contractions(>180mmHg), repetitive contractions, increased LES pressure(>40mmHg). • Hypertensive LES: Increased LES pressure (>40mmHg). Significance of this is questionable.
Endoscopy • Exclude mechanical and inflammatory lesions that are causing dysmotility, structural cause of obstruction. • Endoscopic US still investigational in managing achalasia, used to assist in botulinum toxin injection.
Pharmacological Treatment • Smooth muscle relaxants including Ca channel blockers, nitrates. Also used, anticholinergics, amyl nitrite, NTG, theophylline, ,beta-2-agonists. Experience with these are limited in comparison to the first two.
Pharmacological Treatment • Spastic Disorders: antireflux therapy, TCA, trazodone. • Botulinum toxin injection: into the LES used to treat pts with achalasia. A potent inhibitor of ach release from nerve terminals. May be a good alternative for poor surgical candidates, disadvantage is high cost and need for repeated injections.
Endoscopic Therapy • EGD with pneumatic dilatation is the standard for achalasia. Forceful distension of the LES to 3cm with disruption of the circular muscle layer is needed for symptomatic relief. • Complication is perforation (8%) • If pressure after is less than 10mmHg, outcome excellent.
Surgical Care • Surgical treatments target the LES to relieve the high pressure. • Heller myotomy is procedure of choice for achalasia. It decreases the LES pressure across GE junction and eliminates dysphagia. • Myotomy may lead to GE reflux, so a fundoplication may be necessary with the myotomy.
Surgical Care • Heller myotomy is performed thru either transthoracic or transabdominal approaches. • Efficacy is 60-100% in different series.
Surgical Care • Esophagectomy with gastric pull up or intestinal interposition for patients with advanced disease or refractory cases, unresolved symptoms, carcinoma, perforation during dilation. • Extended Heller Myotomy last resort for DES when pain or dysphagia is severe. • Operation is a myotomy that starts at the LES and goes to thoracic inlet.