Download
1 / 12
120 likes | 364 Views
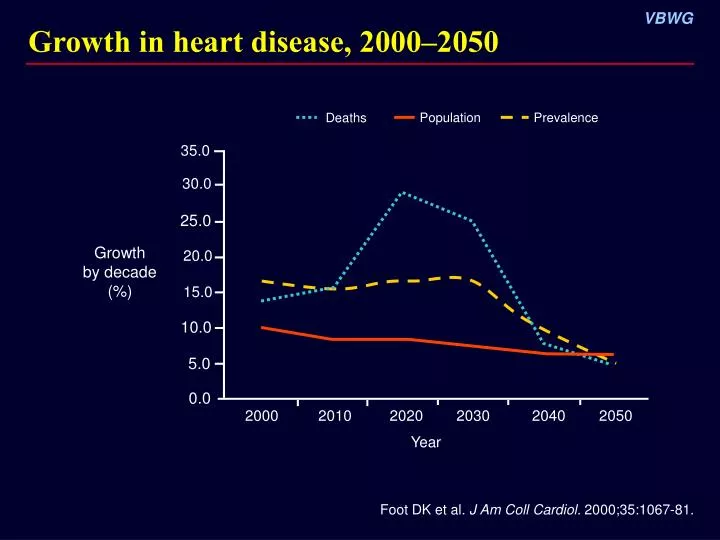
Growth in heart disease, 2000–2050. Population. Prevalence. Deaths. 35.0. 30.0. 25.0. Growth by decade (%). 20.0. 15.0. 10.0. 5.0. 0.0. 2000. 2010. 2020. 2030. 2040. 2050. Year. Foot DK et al. J Am Coll Cardiol. 2000;35:1067-81. Burden of adult hypertension.

E N D
Growth in heart disease, 2000–2050 Population Prevalence Deaths 35.0 30.0 25.0 Growthby decade(%) 20.0 15.0 10.0 5.0 0.0 2000 2010 2020 2030 2040 2050 Year Foot DK et al. J Am Coll Cardiol. 2000;35:1067-81.
Burden of adult hypertension Comparison of NHANES data 1988–1994 and 1999–2000 Hypertensive* P < 0.001 80 History of hypertension** 70 65.2 60 Hypertensive adults (millions) 50.0 50 40 30 20 42.3 59.2 10 7.7 6.0 0 1988–1994 1999–2000 *US adults with SBP ≥140 mm Hg, DBP ≥90 mm Hg, or using antihypertensive medication (conventional definition) **US adults not classified by conventional definition but told at least twice by a healthcare professional that they had high BP Fields LE et al. Hypertension. 2004;44:398-404.
CAMELOT: Optimal BP control in CAD patients Study design: Randomized, double-blind, multicenter, 24-month trial in patients with angiographically documented CAD (N = 1991) Treatment: Amlodipine (10 mg), enalapril (20 mg), or placebo added to background therapy with -blockers and/or diuretics Primary outcome: Incidence of CV events for amlodipine vs placebo IVUS substudy: Measurement of atherosclerosis progression using IVUS (n = 274) Outcome: Change in percent atheroma volume Nissen SE et al. JAMA. 2004;292:2217-26.
CAMELOT: Baseline characteristics and concomitant medications Nissen SE et al. JAMA. 2004;292:2217-26.
CAMELOT: Similar BP reductions frombaseline with amlodipine and enalapril Placebo Amlodipine Enalapril Systolic BP Diastolic BP 132 80 130 78 128 mm Hg P < 0.001 126 P < 0.001 76 124 122 74 120 118 72 0 1 3 6 9 12 15 18 21 24 0 1 3 6 9 12 15 18 21 24 Months Months Nissen SE et al. JAMA. 2004;292:2217-26.
CAMELOT: 31% Reduction in primary outcome with amlodipine compared to standard care 0.25 Placebo Enalapril Amlodipine 31% Relative risk reduction P = 0.003 0.20 0.15 Cumulative CV events (proportion) 0.10 0.05 0 0 18 24 6 12 Months Nissen SE et al. JAMA. 2004;292:2217-26. Primary outcome = incidence of CV events
CAMELOT: Reduction in primary outcome with amlodipine, by subgroup RRR (%) 33.9 4.1 22.9 49.3 26.8 42.8 32.2 29.6 30.9 P 0.002 0.91 0.07 0.006 0.03 0.03 0.03 0.04 0.003 Favors Favors amlodipine placebo Lipid-lowering therapy With statin Without statin Age, y <65 ≥65 Sex Male Female Systolic BP ≤Mean >Mean All patients 0.25 0.5 0.75 1.0 1.25 1.5 Hazard ratio (95% CI) Box size indicates proportion of total study population (ie, smaller boxes have fewer patients relative to other subgroups). Nissen SE et al. JAMA. 2004;292:2217-26.
CAMELOT: Slowed progression of atheroma with amlodipine and enalapril Atheroma volume measured using IVUS at baseline and 24 months (n = 274) All patients Baseline systolic BP > mean P = 0.02 † 2.5 2.3 2.0 Change in percent atheroma volume vs baseline (%) 1.5 * 1.3 1.0 0.8 0.8 0.5 0.5 0.2 0.0 Placebo (n = 95) Enalapril (n = 88) Amlodipine (n = 91) Placebo (n = 49) Enalapril (n = 40) Amlodipine (n = 47) *P = 0.001 vs baseline †P < 0.001 vs baseline Nissen SE et al. JAMA. 2004;292:2217-26.
CAMELOT: Continuous relationship between rate of atheroma progression and change in SBP LOWESS plot for combined amlodipine and enalapril drug-treatment groups 2.5 95% CI 2.0 Progression 1.5 Amlodipine and enalapril groups 1.0 Change in percent atheroma volume (%) 0.5 95% CI 0 –0.5 –1.0 Regression –1.5 –2.0 –40 –30 –20 –10 0 10 20 Change in systolic BP (mm Hg) LOWESS = locally weighted scatterplot smoothing Nissen SE et al. JAMA. 2004;292:2217-26.
INVEST: Similar BP control with CAS and NCAS in hypertensive CAD patients 180 Calcium antagonist strategy (CAS) Noncalcium antagonist strategy (NCAS) 170 160 150 Systolic BP (mm Hg) 140 130 120 110 100 90 Diastolic BP (mm Hg) 80 70 60 0 6 12 18 24 30 36 42 48 Months No. of patients Pepine CJ et al. JAMA. 2003;290:2805-15.
INVEST: Similar reduction in primary outcome with CAS and NCAS in CAD patients 25 Noncalcium antagonist strategy (NCAS) Calcium antagonist strategy (CAS) 20 15 P = 0.057 Cumulative events (%) 10 5 0 0 6 12 18 24 30 36 42 48 54 60 Months No. at risk Primary outcome = first occurrence of death, nonfatal MI, or nonfatal stroke Pepine CJ et al. JAMA. 2003;290:2805-15.
CAMELOT: Conclusions • In CAD patients with “normal” BP, amlodipine demonstrated a significant reduction in ischemia-related CV events. • IVUS substudy showed that progression of coronary atherosclerosis may be minimized or slowed when BP is further reduced below the so-called normal level. • Results suggest optimal BP range for CAD patients may be substantially lower than indicated by current guidelines. Nissen SE et al. JAMA. 2004;292:2217-26.