Download
1 / 26
280 likes | 585 Views
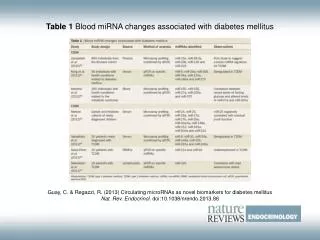
Tamoxifen associated changes. endometrial hyperplasia : can occur in ~1-20% of women treated endometrial polyps : can occur in ~8-36% of women in treated endometrial carcinoma cystic endometrial atrophy . Ultrasound.

E N D
endometrial hyperplasia: can occur in ~1-20% of women treated • endometrial polyps: can occur in ~8-36% of women in treated • endometrial carcinoma • cystic endometrial atrophy
Ultrasound • Tamoxifen may cause the endometrium to appear thickened, irregular, and cystic. Changes tend to be subendometrial in location and cause subendometrial cysts that can be demonstrated at an ultrasound. • Most patients tend to have a multiplicity of findings. According to one study, ~50% of sonograms in those on Tamoxifen revealed an endometrial thickness of 8 mm or more 2. • It has also been reported that the degree of endometrial thickening corresponds to the duration of Tamoxifen therapy.
Ultrasound screening of asymptomatic patients taking tamoxifen has been shown to be problematic due to a high number of false positives. It has been proposed that patients taking tamoxifen who present with vaginal bleeding should go directly to hysteroscopy and endometrial biopsy 7
Postmenopausal women taking tamoxifen should be closely monitored for symptoms of endometrial hyperplasia or cancer. Premenopausal women treated with tamoxifen have no known increased risk of uterine cancer and require no additional monitoring beyond routine gynecologic care. Unless the patient has been identified to be at high risk of endometrial cancer, routine endometrial surveillance has not proved to be effective in increasing the early detection of endometrial cancer in women using tamoxifen and is not recommended.
. Correlation is poor between ultrasonographic measurements of endometrial thickness and abnormal pathology in asymptomatic tamoxifen users because of tamoxifen-induced subepithelial stromal hypertrophy (12). In asymptomatic women using tamoxifen, screening for endometrial cancer with routine transvaginal ultrasonography, endometrial biopsy, or both has not been shown to be effective . • Although asymptomatic postmenopausal tamoxifen-treated women should not have routine testing to diagnose endometrial pathology, sonohysterography has improved the accuracy of ultrasonography in excluding or detecting anatomic changes, when necessary
There is an increased risk of endometrial polyp formation secondary to tamoxifen use for both premenopausal and postmenopausal women
Patients still having a menstrual cycle during tamoxifen had high risk (58.33%) of developing ovarian cysts. We have described an association between pre-menopausal patients using tamoxifen with high E2 level and ovarian cyst enlargement.
Effect of tamoxifen on the uterus • Tamoxifen results in a spectrum of uterine abnormalities including benign alterations such as endometrial polyps, endometrial hyperplasia, endometrial cystic atrophy, adenomyosis, and uterine fibroid growth as well as malignant transformation into endometrial carcinoma and uterine sarcoma
Leiomyomas • Several studies have demonstrated a growth of uterine fibroids in postmenopausal patients treated with tamoxifen. • However, the leiomyomas in women treated with tamoxifen do not appear to differ histologically from those in untreated women
Asymptomatic unilocular cysts in these patients should be followed conservatively and discontinuation of tamoxifen usually leads to the reduction and disappearance of these cysts[50]. One study found women taking tamoxifen for less than 2 years were not at increased risk of ovarian cancer[52]. Of particular concern is the negative effect of tamoxifen-induced ovulation and the risk of ovarian carcinoma in patients with BRCA1 and BRCA2 gene mutations. Annual sonographic monitoring of the ovaries in this population has been recommended although its efficacy is still unproven
Effect of tamoxifen on the cervix • Women treated with tamoxifen have a higher incidence of benign reactive atypia or atypical squamous cells of undetermined significance, without an increase in dysplasia or cervical cancer
The normal postmenopausal endometrium appears as a single echogenic line and should not exceed 5 mm as a bilayer thickness[60,61]. Most women undergoing tamoxifen treatment have a thicker endometrium compared with control subjects (9–13 mm versus 4.0–5.4 mm)[10–12,62]. In postmenopausal women undergoing estrogen replacement therapy, the normal endometrium may measure up to 8 mm in thickness.
Various authors have recommended endometrial thickness cut-off values ranging from 4 to 10 mm with sensitivity of positive histologic findings ranging from 85 to 100% and specificity ranging from 56 to 96% • a thicker endometrium on the US image does not necessarily correlate with specific pathologic endometrial findings
the most common endometrial transvaginal US pattern seen in women treated with tamoxifen is a thickened endometrium with cystic spaces described as a ‘Swiss cheese’ pattern[10–12,27,71–76] (Fig. 1). The findings of a thickened endometrial complex, with or without cystic changes, is often non-specific and may be caused by endometrial polyps, submucosal leiomyoma, cystic atrophy, endometrial hyperplasia, or carcinoma
Sagittal transvaginal ultrasound images from three different patients show the most common endometrial finding in women undergoing tamoxifen treatment: a thickened endometrium with cystic spaces.
Sagittal transvaginal ultrasound :a thickened endometrium. Sagittal hysterosonogram showed no evidence of endometrial mass or thickening. The apparent thickening on the transvaginal ultrasound was secondary to subendometrial/myometrial cysts.
Polyps often have a narrow attachment to the endometrium but may be broad-based (Fig. 3). Submucosal fibroids appear as round structures arising from the myometrium, commonly with wide attachment to the myometrium, although they are occasionally pedunculated. Hysterosonographic features of adenomyosis include small cysts which appear in the inner myometrium[63]. Diffuse smooth thickening of the endometrium suggests hyperplasia, however, hyperplasia may also appears as irregular asymmetric endometrial thickening[86]. An irregular heterogenous mass or irregular focal thickening of the endometrium is suggestive of endometrial carcinoma
Sagittal transvaginal ultrasound demonstrates a markedly thickened, heterogeneous endometrium. • (b) Transverse view from hysterosonogram demonstrates irregular thickening with of the endometrium with internal vascularity which was found to represent endometrial carcinoma.
Doppler • in the majority of studies Doppler indices have been unable to differentiate between benign and pathologic etiologies. • In certain cases, color Doppler US can improve the specificity of sonography by showing the feeding artery in the pedicle of a polyp
Asymptomatic women can then be screened annually with transvaginal ultrasound from 1 to 2 years after the start of tamoxifen. The strength of transvaginal US is in the normal findings. In cases where the transvaginal US image is non-diagnostic or is suggestive of an abnormality, hysterosonography can provide additional information.
in cases with ovarian cyst formation during tamoxifen treatment of breast cancer, discontinuation of tamoxifen and administration of GnRH is quite a reasonable way to proceed in most patients. Surgical intervention should be carried out when cysts are persistent, bilateral, large or complex
Transvaginal ultrasonography examination at admission showed a right multilocular ovarian cyst (85×40 mm) and a left multiloculated mass (65×46 mm).