Download
1 / 45
470 likes | 874 Views
Tamoxifen Pharmacogenetics and Prediction of Breast Cancer Relapse After Administration of Tamoxifen. Matthew P. Goetz, MD Assistant Professor of Oncology Mayo Clinic College of Medicine. David Flockhart, MD, PhD

E N D
Tamoxifen Pharmacogenetics and Prediction of Breast Cancer Relapse After Administration of Tamoxifen Matthew P. Goetz, MD Assistant Professor of Oncology Mayo Clinic College of Medicine David Flockhart, MD, PhD Consortium on Breast Cancer Pharmacogenomics (COBRA) Pharmacogenomics Research Network CP1229323-1
Invasive Breast Cancer: 212,920 New Cases Ductal Carcinoma in Situ: 61,980 Cases 2/3 are estrogen positive—Candidates for hormonal therapy Breast Cancer2006 (USA) Jemal A, et al. CA Cancer J Clin 2006;56;106-30
Tamoxifen • The most important drug worldwide for hormone receptor positive breast cancer • Approved by the FDA for treatment of • High-risk patients • DCIS • Pre and Postmenopausal breast cancer • Metastatic disease • Most commonly used hormonal therapy in early and advanced male breast cancer CP1229323-2
Tamoxifen and Breast Cancer FDA-Approved Indications Adjuvant Postmenopausal Node+ Postmenopausal Metastatic Premenopausal Metastatic Adjuvant Node-negative Male Metastatic “Prevention” DCIS 1977 ‘89 ‘90 ‘93 ‘86 ‘98 2000
Tamoxifen (for ~5 yrs) in Early Breast Cancer Oxford Meta-analysis* Control 45-0% 38.3 Hazard Ratio (Control/Tamoxifen) = ~1.69 26.5 Recurrence (%) 24.7 About 5 years of tamoxifen 33.2% 15.1 Years *10,386 women EBCTCG: Lancet 365:1687, 2005 CP1193154-1
R R R Adjuvant Hormonal Therapy: Designs of Recent Major Trials Extended Adjuvant Therapy DFS HR 0.57 5 yr ~5 yr Switching DFS HR 0.68 Tamoxifen 2-3 yr 2-3 yr 5 yr Aromatase Inhibitor Initial Adjuvant Therapy Placebo DFS HR 0.83 CP1157143-1
Pre-menopausal Tamoxifen for 5 years Postmenopausal Aromatase inhibitor for 5 years or… Tamoxifen for 2-3 yrs followed by an AI Adjuvant hormonal therapy
20 15 10 5 Anastrozole Tamoxifen 0 ATAC: Recurrences before 2.5 years HR 95% CI p-value AN vs TAM 0.78 0.65–0.93 0.007 Absolute difference 1.6% Proportion with recurrence (%) 0 0 6 12 18 24 30 36 42 48 54 No. of Pts. at risk Time to event (months) AN TAM 2617 2598 2533 2516 2436 2386 2243 2180 1258 1210 602 574 Howell A, EBCC Hamburg 3-18-2004 * Censoring non-BC deaths before recurrence
Is there a better way to identify patients for whom tamoxifen or anastrozole would be the preferred drug for initial adjuvant endocrine therapy?
Tamoxifen Metabolic Pathway CP1229323-3 Jin, Y. et al. J Natl Cancer Inst 2005;97:30-39
Endoxifen and 4-OH-Tamoxifen are Equipotent as Inhibitors of Estrogen Stimulated Cell Proliferation Cell Growth Concentration Johnson MD, et al: Breast Cancer Res Treat 85:151-9, 2004
Same potency in ERbinding1 Suppression of ER-dependent MCF-7 proliferation2 global ER-responsive gene expression3 Different Endoxifen concentrations 10 fold higher than 4-hydroxy tamoxifen4 Endoxifen and 4-OH tamoxifen 1. Johnson et al. Breast Cancer Res Treat 2004. 2. Lim YC, Cancer Chemother Pharmacol 2005;. 3. Lim YC, et al. J Pharmacol Exp Ther 2006;In Press. 4. Stearns Vet al. J Natl Cancer Inst 2003.
Tamoxifen Metabolic Pathway Jin Y et al: J Natl Cancer Inst 97:30, 2005 CP1229323-3
CYP2D6 Genotype and Endoxifen P<0.001, r2=0.24 Plasma Endoxifen (nM) CYP2D6*4 (most common genetic variant associated with the CYP2D6 poor metabolizer state) Jin Y et al: J Natl Cancer Inst 97:30, 2005 CP1229323-4
NCCTG 89-30-52 RANDOMIZATION 5 years of tamoxifen(n=256) Postmenopausal women Early ER+ breast cancer 541 women accrued 5 years tamoxifen +1 year fluoxymesterone(n=285) Ingle et al. Breast Cancer Res Treat. 2006 Mar 15 CP1229323-5
Surgically resected stage I-III breast cancer All tumors were estrogen receptor positive ≥10 fmol/mg cytosol protein positive or positive by immunohistochemical assay No adjuvant chemotherapy allowed Median follow-up of 11 years Accrual completed in April 1995 No differences in RFS or OS NCCTG 89-30-52 Ingle et al. Breast Cancer Res Treat. 2006 Mar 15
CYP2D6*4 Genotyping • Tamoxifen monotherapy arm (256 patients) • Formalin-fixed paraffin-embedded tumor blocks (223 patients) • CYP2D6*4 (n=190) • Wt/Wt – 137 (72%) • Wt/*4 – 40 (21%) • *4/*4 – 13 (7%) Goetz, Rae et al: J Clin Oncol 23:9312, 2005 CP1229323-6
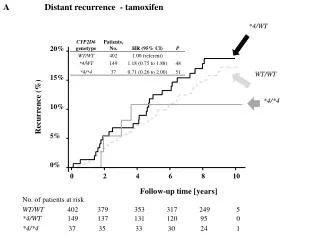
Relapse-free Time CYP2D6 Wt/Wt CYP2D6 *4/Wt CYP2D6 *4/*4 % P=0.030 Years after randomization CP1193836-1 Goetz et al J Clin Oncol. 2005;23(36):9312-8.
Relapse-free Survival CYP2D6 WT/WT % CYP2D6 *4/WT CYP2D6 *4/*4 P=0.020 Years after randomization Goetz et al J Clin Oncol. 2005;23(36):9312-8. CP1193836-2
Incidence of Moderate or Severe Hot Flashes Goetz et al J Clin Oncol. 2005;23(36):9312-8.
CYP2D6 *4 Genotype and Clinical Outcome (multivariate analysis) • *4/*4 vs Wt/Wt or Wt/*4 • Time to breast recurrence: HR* 1.85, p=0.176 • Relapse-free survival: HR* 1.86, p=0.089 * Adjusted for nodal status, tumor size Goetz, Rae et al: J Clin Oncol 23:9312, 2005 CP1229323-7
Without Paroxetine With Paroxetine Stearns V, et al. J Natl Cancer Inst 2003;95(23):1758-64
Inhibition of CYP2D6 Affects Endoxifen Concentrations Plasma Endoxifen (nM) Wt/Wt, noinhibitor Venlafaxine Sertraline Paroxetine *4/*4, noinhibitor Jin Y et al: J Natl Cancer Inst 97:30, 2005 CP1229323-8
CYP2D6 Inhibitors and BreastCancer Relapse • Paroxetine, fluoxetine, and venlafaxine significantly reduce the number and severity of hot flashes in tamoxifen-treated women1-3 • 30% tamoxifen-treated patients are prescribed antidepressants for depression or hot flashes4 • Other commonly administered medications also inhibit CYP2D6 (amiodarone, doxepin, cimetidine) • An analysis of CYP2D6 metabolism in tamoxifen treated patients is incomplete without accounting for CYP2D6 inhibitors 1. Loprinzi CL et al. Lancet 2000;356:2059–63. 2. Loprinzi CL, et al. J Clin Oncol 2002;20:1578–83. 3. Stearns et al. JAMA 2003;289:2827–34. 4. Love et al. Patterns of Care in Medical Oncology (2005) CP1229323-9
NCCTG 89-30-52 RANDOMIZATION 5 years of tamoxifen(n=256) Postmenopausal women Early ER+ breast cancer 541 women accrued 5 years tamoxifen +1 year fluoxymesterone(n=285) Ingle et al. Breast Cancer Res Treat. 2006 Mar 15 CP1229323-5
Methods • 225 Charts were reviewed at each randomizing site to ascertain medication history • Potent CYP2D6 inhibitors: Fluoxetine and paroxetine • Moderate CYP2D6 inhibitors: Sertraline, cimetidine, amiodarone, doxepin, ticlopidine, or haloperidol • Duration of coadministration: <1, 1-2, 2-3, 3-4 and 4-5 years • Statistics: Log rank test and Cox modeling CP1229323-10
CYP2D6 metabolism defined by *4 genotype and medication history Extensive CYP2D6 metabolism Wt/Wt, no inhibitor Decreased CYP26 metabolism Wt/*4 *4/*4 Any genotype and co-administration (yes/no) of a moderate or potent CYP2D6 inhibitor Methods
Patient Characteristics Metabolizer status known n=180 Median age (range) 68 (42-87) ER status (%) 100 Tumor size (cm) <3 (%) 78 3 (%) 22 Positive nodes 0 (%) 64 1-3 (%) 25 4-9 (%) 7 10 (%) 4 Tumor grade 1 (%) 24 2 (%) 54 3 (%) 15 Unknown (%) 7 CP1229323-13 Goetz et al. Breast Cancer Res Treat. 2006 (In press)
Results • CYP2D6 metabolism determined in 180 pts (medication history 225 pts) • Inhibitor status • Potent inhibitors (n=3) • Moderate inhibitors (n=10) • Median duration of use 2-3 years CP1229323-12 Goetz et al. Breast Cancer Res Treat. 2006 (In press)
Time to Breast Recurrence Extensive n=115 Decreased n=65 % P=0.015 Years after randomization CP1234316-1 Goetz et al. Breast Cancer Res Treat. 2006 (In press)
Relapse-Free Survival Extensive n=115 % Decreased n=65 P=0.007 Years after randomization CP1234316-3 Goetz et al. Breast Cancer Res Treat. 2006 (In press)
Overall Survival Extensive n=115 % Decreased n=65 P=0.082 Years after randomization CP1234316-4 Goetz et al. Breast Cancer Res Treat. 2006 (In press)
Outcomes by Metabolizer StatusMultivariate Analysis* Hazard ratio (relative toOutcome extensive metabolizers) P value Time to breast recurrence 1.91 (1.05-3.45) 0.034 Relapse-free survival 1.74 (1.10-2.74) 0.017 Overall survival 1.35 (0.83-2.16) 0.223 *Adjusted for size, grade and nodal status, ER, PR, HER-2 CP1229323-19 Goetz et al. Breast Cancer Res Treat. 2006 (In press)
Inhibition of CYP2D6 Affects Endoxifen Concentrations Plasma Endoxifen (nM) Wt/Wt, noinhibitor Venlafaxine Sertraline Paroxetine *4/*4, noinhibitor Jin Y et al: J Natl Cancer Inst 97:30, 2005 CP1229323-8
Decreased CYP2D6 Metabolism Intermediate metabolizers: n=40 Wt/*4 and no inhibitor (n=32) Wt/Wt and moderate inhibitor (n=8) Poor metabolizers: n=16 4/*4 (n=13) Any genotype and potent inhibitor (n=3) Unknown: n=9 Wt/*4 without med history (n=7) Unknown genotype and mod inhibitor (n=2) CYP2D6 Metabolism by Genotype and Inhibitor Goetz et al. Breast Cancer Res Treat. 2006 (In press)
Time to Breast Recurrence EM n=115 IM n=40 % Log Rank P=0.019 n=16 PM Years after randomization CP1229323-15 Goetz et al. Breast Cancer Res Treat. 2006 (In press)
Relapse-Free Survival n=115 EM 2-year RFS EM 98% IM 92% PM 68% Log Rank P=0.009 % n=40 IM n=16 PM Years after randomization CP1229323-16 Goetz et al. Breast Cancer Res Treat. 2006 (In press)
Overall Survival EM n=115 IM % n=40 n=16 PM Log Rank P=0.145 Years after randomization CP1229323-17 Goetz et al. Breast Cancer Res Treat. 2006 (In press)
Outcomes by Metabolizer StatusUnivariate Analysis Hazard ratio (relative toOutcome extensive metabolizers) P value Time to breast recurrence PM 3.20 (1.37-7.55) 0.007 IM 1.49 (0.68-3.05) 0.338 Relapse-free survival PM 2.69 (1.34-5.37) 0.005 IM 1.63 (0.95-2.78) 0.075 Overall survival PM 2.00 (0.92-4.17) 0.077 IM 1.40 (0.80-2.43) 0.240 Goetz et al. Breast Cancer Res Treat. 2006 (In press) CP1229323-18
ATAC: Smoothed Hazard Rates for RecurrenceHormone Receptor + patients 3.0 2.5 2.0 Annual hazard rates (%) 1.5 1.0 Anastrozole 0.5 Tamoxifen 0 0 1 2 3 4 5 6 Follow-up time (years) Howell, et al. 2004 San Antonio Breast Cancer Symposium
Hazard Rates for RFS by CYP2D6Metabolizer Status (n=180) Decreased Hazard rates Extensive Years after randomization CP1229323-20 Goetz et al. Breast Cancer Res Treat. 2006 (In press)
Conclusion • In this trial, CYP2D6 metabolism was an independent predictor of clinical outcome in postmenopausal women with ER positive early breast cancer • The effect of impaired metabolism was most marked in poor metabolizers • Consistent with clinical data that tamoxifen activation to endoxifen is dependent upon CYP2D6 CP1229323-21
Conclusion • These data suggest that determination of CYP2D6 genotype may be of value in selecting adjuvant hormonal therapy and moderate/potent CYPY2D6 inhibitors should not be co-administered with tamoxifen CP1229323-22
Mayo Clinic Cancer Center North Central Cancer Treatment Group Pharmacogenetics Research Network COBRA : The Consortium for Breast Cancer Pharmacogenomics: Indiana University School of Medicine University of Michigan Johns Hopkins University Mayo Clinic Baylor College of Medicine Mayo Clinic Breast Cancer SPORE Acknowledgments
CYP2D6 Individualized Adjuvant Hormonal Study RANDOMIZE Tam (2.5 years) followed by AI (2.5 years) (n=1950) EM, UM Postmenopausal women ER positive breast cancer UM: Ultra-rapid Metabolizer EM: Extensive Metabolizer IM: Intermediate Metabolizer PM: Poor Metabolizer CYP2D6 Genotyping AI (5 years total) (n=1950) IM, PM Standard of care (AI for 5 years) CYP2D6 IM, and PM: heterozygous or homozygous for *3, *4, *5, *6, *7, *8, *11, *12