Download
1 / 25
250 likes | 430 Views
Organ Donor Incentives and Preferences. Adrienne Janney April 15, 2005 SI 646: Information Economics. Outline. Why organ donation Organ allocation Addressing organ scarcity Cadaveric donation Incentive-minded policies To opt in or to opt out? Recommendation Questions.

E N D
Organ Donor Incentives and Preferences Adrienne Janney April 15, 2005 SI 646: Information Economics
Outline • Why organ donation • Organ allocation • Addressing organ scarcity • Cadaveric donation • Incentive-minded policies • To opt in or to opt out? • Recommendation • Questions
Organ donation: ‘The Gift of Life’ • Organs are scarce goods • Waitlisted as of last night: 88,212 • Transplants YTD as of last week: 2,271 from 1,164 donors, living or dead • In 2003, 7,147 people died of 114,442 waiting for organs • In 2000, the MTT was 1,199 days (3.28 years) • Organs are indivisible goods (houses) • Kidneys come in pairs • Livers and pancreases can be split • Everyone comes with one set of organs (there’s no ‘organ manufacturing plant’) • Organs are not cakes Source: United Network for Organ Sharing
Organ donation: Allocation methods • Markets • Standing in line (queue) • Rationing • Lottery • Auction (Thanks, Jeff)
Organ donation: Allocation methods • Markets • Standing in line (queue) • Rationing • Lottery • Auction (Thanks, Jeff)
Organ donation: Allocation methods • Markets • Standing in line (queue) • Rationing • Lottery • Auction (Thanks, Jeff)
Organ allocation: UNOS • Rationing + queue + lottery (at the top) • Waiting list • Numerical medical score based on laboratory findings • Time on list counts in a tie • Divided up by region (for efficiency—organ viability) • Requires blood type and possibly histologic tissue match • Compliance matters • ‘Pull’ doesn’t matter (rich & famous) • Note: requires insurance—private or Medicare or Medicaid
Addressing the scarcity: Ideas • Increase cadaver pool • Increase living donor pool • Stem cell research (growing transplant organs) • Artificial organs/organ ‘replacement’ technology (e.g., hemodialysis)
Addressing the scarcity: Problems • Cadaver pool increasing at slow rate • Living donation only addresses certain organs (kidneys and sometimes liver or pancreas) • Stem cell research funding support decreasing—and it’s a long way off • Not yet developed, and so far less quality of life with external mechanisms
Deceased and Living Donors1994-2003 Source: United Network for Organ Sharing
Live donors on increase Innovation Kidney exchange ‘housing’ problem Only addresses some organs (worth saying again) Less chance of rejection/graft failure for organ recipient Addressing the scarcity: Live donors
Addressing the scarcity: Live donors • Donor incurs risk and costs • Death • Pain • Temporary but dramatic illness • Less organs to spare • Unsuccessful donation (transplant outcome=death) • Time off work/downtime
(Interlude: Pareto efficiency) • Recipients benefit from any donor • Live donors incur risk/costs • Ex-post donors lose and gain nothing • Cadaver donation as Pareto efficient? • But: Live donors gain utility via altruism • Jeff says: Dead men don’t have a utility distribution.
Cadaveric donation: Barriers • People don’t want to think about death • You have to opt in (more on this later) • Family ability to override (in some states) • Family asked at a time of newly inflicted grief (fear of regret, high emotional state)
Cadaveric donation: Ex-ante costs • Taking an action (phone, mail, e-mail, forms) • Psychic costs (upsetting) • Cognitive costs • Cost of processing new information • Cost of changing viewpoint • Social costs (explaining/convincing family)
Cadaveric donation: Education • (Advertising) • Education campaigns have not pushed donation rates to critical mass • Possible reasons? • Lack of quality? • Not ‘values’ driven • Lack of quantity? • Not reaching enough people • Futile venue for offsetting associated costs?
Incentive-minded policies • Tax incentives • Donor must be able to realize benefit ex-ante • Enforcement issues dictate ex-post payoff • Money to family or burial • Not in use in the United States • ‘Donor will’ • Family cannot override donor-stated preference • Emphasizes individual choice (an American value) • # of states currently implementing • E.g.: Indiana transplants livers at a lower MELD score (better chances of translant), but still a significant shortage
To opt in, or to opt out? • We have opt in (‘explicit consent’) • You have to volunteer your preference to be an organ donor • And in many states your family has to agree • Misclassification potential: underutilization • Several countries have tried opt out (‘presumed consent’) • Everyone presumed to be a donor • Individuals may opt out at any time by own initiative • Usual exclusions: minors, prisoners, mentally ill • Misclassification potential: unwilling donors donate
To opt in, or to opt out? • Classical economics: policy defaults have limited effects • However, ‘constructed’ preference research implies otherwise • For unexpressed preferences, defaults do matter Source: Johnson and Golsdtein (2003)
To opt in, or to opt out? • Defaults influences decisions • Decision-makers believe defaults are suggestions • Making a decision involves effort (accepting default is effortless) • Defaults often represent status quo; change usually involves tradeoff • ‘Loss aversion’ • “Loss looms larger than equivalent gains” Source: Johnson and Golsdtein (2003)
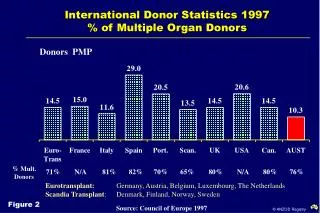
To opt in, or to opt out? Opt out countries & rates of consent (%) Source: Johnson and Golsdtein (2003)
To opt in, or to opt out? Opt in countries and rates of consent (%) Source: Johnson and Golsdtein (2003)
To opt in, or to opt out? • ‘Natural experiments’ with organ donation and opt in/opt out • Revealed donation rates twice as high when opting out as in • Neutral condition (reveals true preferences?) • Not far off from opt-out rate, implying true preferences may be closer to opt-out result Source: Johnson and Golsdtein (2003)
Policy recommendation Adopting presumed consent in United States will increase cadaver pool, take pressure off waiting list and live donor supply, and install a policy default that provides incentive to donate by reducing costs association with making and affirming decisions.
Questions? • Does this system reveal true preferences? • Problems? • Better systems? • Ethical considerations? • Missed information issues? • Botched economics? • Your questions.