Download
1 / 87
870 likes | 893 Views
This topic explores the structure and function of the heart, including its size, location, chambers, valves, and blood supply. It also covers common valve disorders and the importance of the fibrous skeleton.

E N D
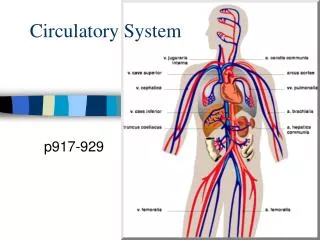
Biology 221 Anatomy & Physiology II TOPIC 2 Circulatory System – The Heart Chapter 18 pp. 675-710 E. Lathrop-Davis / E. Gorski / S. Kabrhel Interactive Physiology: Cardiovascular System
N Function & Size • Function: provide pressure for movement of blood through blood vessels by alternately contracting (systole) and relaxing (diastole) • Size • 250 – 350 grams • extends from 2nd rib to 5th intercostal space
Location • within the pericardial cavity in mediastinum of the thoracic cavity • directly posterior to the sternum, ~2/3 lies left of midline Fig. 18.1, p. 677
N Pericardium & Pericardial Cavity • Fibrous pericardium – outer layer of pericardial sac • stabilizes heart in mediastinum • Serous pericardium • parietal layer • visceral layer = epicardium http://www.cyber-nurse.com/veetac/horrorctam.htm
N Pericardium & Pericardial Cavity • Pericardial cavity • pericardial fluid • Pericarditis – inflammation of the pericardium • normally hinders production of serous fluid • cardiac tamponade –fluid in pericardial cavity increases http://www.cyber-nurse.com/veetac/horrorctam.htm http://www.cyber-nurse.com/veetac/horrorctam.htm
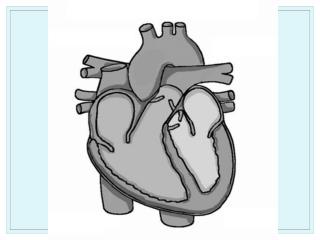
N Chambers of the Heart • 2 Atria – receive blood from veins • auricles – fill with blood from venae cavae • coronary sulcus = atrioventricular groove • interatrial septum • fossa ovalis – remnant of foramen ovale • pectinate muscles • Base Fig. 18.4b p. 679
N Chambers of the Heart • 2 Ventricles pump blood into arteries • anterior interventricular groove • posterior interventricular groove • interventricular septum • papillary muscles attach to chordae tendineae • trabeculae carneae • Apex Fig. 18.4b p. 679
Structure of the Heart Wall Composed of 3 layers: • Epicardium = visceral pericardium • Myocardium • Endocardium Fig. 18.2, p. 677 http://www.cyber-nurse.com/veetac/horrorctam.htm
N Structure of the Heart Wall • Epicardium = visceral pericardium • serous membrane • mesothelium • areolar connective tissue • adipose accumulates in grooves • Myocardium • cardiac muscle, blood vessels and nerves • fibrous skeleton • Endocardium – endothelium Fig. 18.2, p. 677
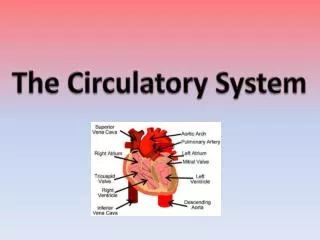
N Great Vessels of Heart Arteries – carry blood away from heart • pulmonary artery (trunk) – pulmonary circ. • aorta – systemic circulation Fig. 18.4, p. 679-680
N Great Vessels of Heart Veins – return blood to heart • pulmonary veins – pulmonary circulation • superior & inferior venae cavae – systemic circulation • coronary sinus and other coronary veins - coronary circulation Fig. 18.4, p. 679-680
N Atrioventricular (AV) Valves • allow blood to flow from atria to ventricles when latter are relaxing • prevent flow from ventricles to atria when ventricles are contracting* • mitral (bicuspid) • tricuspid Fig. 18.8, p. 685 Return to cardiac cycle
N Semilunar (SL) Valves • allow blood to flow from ventricles to arteries when ventricles are contracting • prevent back flow from arteries to ventricles when ventricles relax* Fig. 18.8, p. 685 Fig. 18.4, p. 681 Return to cardiac cycle
N Heart Sounds • Normal sounds - closure of valves • “lub” – closure of AV valves • “dup” –closure of semilunar valves Fig. 18.19, p. 695
N Valve Disorders • Rheumatic heart disease (RHD) – strep (Streptococcus pyogenes) infection leads to inflammation of heart and valves; heart valves become stiffened into partially closed position • Murmur – abnormal heart sound associated with bad valves • incompetance – damaged valve allows backflow of blood • stenosis – narrowing of passageway through valve
Fibrous Skeleton • Internal connective tissue framework • Functions include: • stabilizes positions of muscle cells and valves • supports muscle cells, blood vessels, nerves • helps spread force of contraction through heart • prevents over-distention • helps maintain shape of heart • physically and electrically separates atrial and ventricular musculatures
Cardiac Anatomy Review, pp. 8-9 N Microanatomy of the Myocardium • Cardiac muscle • short, branching, uninucleate cells • striated – sliding filament movement • Connected by intercalated discs • gap junctions • functional syncytium • desmosomes • Numerous large mitochondria • aerobic respiration • high O2 demand • myoglobin http://www.usc.edu/hsc/dental/ghisto/musc/c_20.html Fig. 18.11, p. 688
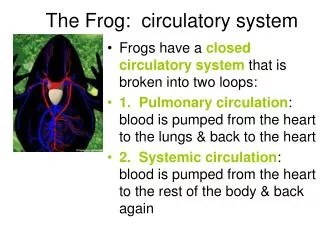
Cardiac Anatomy Review, pp. 6-7 N Blood Flow Through the Heart • Pulmonary – to and from capillary beds associated with alveoli of lungs • brings deoxygenated blood to lungs; returns oxygenated blood to heart • Systemic – to and from capillary beds of the tissues of the body • brings oxygenated blood to tissues; returns deoxygenated blood to heart Fig. 18.5 p. 682
N Coronary Blood Supply • Anastomoses – provide collateral circulation • Blood enters coronary vessels during diastole, empties during systole • Autoregulation – coronary arteries dilate when demand for nutrients and oxygen increases • Capillaries present in endomysium (endo = within; mysium = muscle) • areolar CT within intracellular space between muscle cells • endomysium connected to fibrous skeleton
Coronary Blood Supply: Arteries • Branches of aorta • Supply oxygen-rich blood to myocardium • Right coronary artery • branches serve right atrium and right ventricle, SA and AV nodes, and posterior walls of both ventricles Fig. 18.7, p. 683
Coronary Blood Supply: Arteries • Left coronary artery • branches serve interventricular septum and anterior walls of both ventricles, left atrium and posterior wall of left ventricle • branches into anterior interventricular artery and circumflex artery Fig. 18.7, p. 683
N Coronary Circulation: Veins • Coronary Sinus • great cardiac vein - drains area supplied by anterior interventricular artery • other left and posterior coronary veins - drain left side and posterior of heart • Anterior cardiac veins – drain anterior surface of right ventricle Fig. 18.7, p. 683 Fig. 18.4, p. 679
Coronary Circulation: Disorders • Occlusion – blockage; in a vessel, tissue downstream will be deprived of oxygen and nutrients • Ischemia – transient state of oxygen deficit leading to reversible changes in cell structure and function • Infarction – localized area of cell death (necrosis) resulting from anoxia; causes include • disruption of arterial circulation serving the area • disruption of venous drainage
N Comparison with Skeletal Muscle • All-or-none law - either an event occurs completely (e.g., contraction) or it does not (no partial contraction) • in skeletal muscle, applies to motor units • in cardiac muscle, applies to entire organ • Length of absolute refractory period • skeletal muscle – 1-2 ms allows tetanus • cardiac muscle ~ 250 ms prevents tetanus Fig. 18.12, p. 689
N Comparison with Skeletal Muscle Means of stimulation • skeletal muscle – only contracts in response to stimulation by somatic motor neuron • cardiac muscle • certain cells are self-excitatory = autorhythmicity • autonomic innervation changes rate of depolarization • sympathetic innervation increases rate • parasympathetic innervation decreases rate • also responds to epinephrine
Cardiac Action Potential, p. 3 Types of Cardiac Muscle Cells Autorhythmic cardiac muscle cells • capable of spontaneously depolarizing to produce pacemaker potentials • conduct action potentials through myocardium • not contractile • form intrinsic conduction system
Cardiac Action Potential, p. 4 Types of Cardiac Muscle Cells Contractile cardiac muscle cells • depolarization spreads from autorhythmic cells via gap junctions • action potential leads to contraction as myofilaments slide past each other • responsible for alternating contraction (systole) and relaxation (diastole) that creates pressure on blood
Cardiac Action Potential, p. 5 Conduction Through the Heart • Action potential spreads rapidly through conduction system and contractile cells via gap junctions • Atria and ventricles functionally separated by fibrous skeleton • Time to total depolarization ~ 220 ms (~0.22s) in a healthy heart
Cardiac Action Potential, p. 6-10 N AP: Autorhythmic Cells - Overview • Ion channels allow ion movements • Na+ ( Na+/K+) leakage channels • Voltage-gated K+ channels • Voltage-gated Ca2+ channels • Ion movements affect membrane potential • Resting membrane potential is negative Fig. 18.13, p. 697
Cardiac Action Potential, p. 6-10 AP: Autorhythmic Cells - Steps • Pacemaker potential • Action potential depolarization • Action potential repolarization Fig. 18.13, p. 697
Cardiac Action Potential, p. 6-10 N Autorhythmic AP:Pacemaker Potential • gradual change in membrane potential from resting (- 60 to -70 mV) toward threshold • Na+ channels open net gain of + charge slow depolarization = pacemaker potential • closure of voltage-gated K+ channels contributes to slow depolarization Fig. 18.13, p. 697
Cardiac Action Potential, p. 6-10 Autorhythmic AP: Depolarization • at threshold (~ -40 mV), voltage-gated Ca2+ channels open Ca2+ enters from extracellular fluid rapid depolarization of action potential Fig. 18.13, p. 697
Cardiac Action Potential, p. 6-10 N Autorhythmic AP: Repolarization • depolarization causes voltage-gated K+ channels to open K+ leaves cell repolarizes • decrease in voltage causes Ca2+ channels to close, aids repolarization • after a while, K+ channels start to close, Na+ channels open; cycle starts over • Na+/K+ pump Fig. 18.13, p. 697
Cardiac Action Potential, p. 11 AP: Contractile Cells • Connected to autorhythmic cells by gap junctions • Ion channels allow ion movements • Voltage-gated Na+ channels • Voltage-gated K+ channels • Voltage-gated Ca2+ channels • Resting membrane potential is negative Fig. 18.12, p. 689
Cardiac Action Potential, p. 12-17 AP: Contractile Cells - Steps • Depolarization • Plateau • Repolarization Fig. 18.12, p. 689
Cardiac Action Potential, p. 12-17 N Contractile AP: Depolarization • Sodium (and calcium) ions pass from autorhythmic cells via gap junctions • Contractile cell depolarizes from resting to threshold • At threshold, fast voltage-gated sodium channels open Na+ rushes in depolarization to ~ +30 mV Fig. 18.12, p. 689
Cardiac Action Potential, p. 12-17 N Contractile AP: Plateau • After a short time, Na+ channels close and voltage-gated K+ channels open membrane potential begins to fall • Voltage-gated Ca2+ channels also open and allow Ca2+ influx • Ca2+ influx balances K+ efflux (channels close temporarily) resulting in plateau Fig. 18.12, p. 689
Cardiac Action Potential, p. 12-17 N Contractile AP: Plateau • combination of Ca2+ influx and inactivation of K+ channels results in plateau, coupled with slow return of Na+ channels to ready position results in long absolute refractory period • Why would this be important to heart function? • Ca2+ influx causes contraction Fig. 18.12, p. 689
Cardiac Action Potential, p. 12-17 Contractile AP: Repolarization • rapid repolarization occurs as Ca2+ channels close and K+ channels reopen • K+ influx returns membrane to resting potential • Ca2+ actively transported out of cell and into sarcoplasmic reticulum • Na+/K+ pump restores ion levels to resting Fig. 18.12, p. 689
Intrinsic Conduction System, pp. 3-4 Electrical Conduction - Overview sinoatrial (SA) node internodal pathway to atrioventricular (AV) node & atria atrioventricular (AV) bundle (bundle of His) right and left bundle branches Purkinje fibers ventricles (starting at apex) Fig. 18.14, p. 691
Intrinsic Conduction System, pp. 3-4 Conduction Pathway: SA Node • Sinoatrial (SA) Node • located in right atrial wall, inferior to opening of superior vena cava • acts as normal pacemaker sinus rhythm • intrinsic rate ~ 100 APs/min • ~ 75 APs / min at rest under normal hormonal and neural control • resting HR varies; more fit, slower heart rate • AP spreads to atria and to AV node via internodal pathway Fig. 18.14, p. 691
Intrinsic Conduction System, pp. 3-4 Conduction Pathway: AV Node • Atrioventricular (AV) Node • located in inferior interatrial septum above tricuspid valve • connects atria and ventricles • short delay (~ 0.1 s) -- Why is this delay important?
Intrinsic Conduction System, pp. 3-4 Conduction Pathway: AV Bundle • Atrioventricular (AV) Bundle (bundle of His) • Right and Left Bundle Branches • run through interventricular septum toward apex of heart Fig. 18.14, p. 691 Fig. 18.17, p. 694
Intrinsic Conduction System, pp. 3-4 N Conduction Pathway: Purkinje Fibers • run through interventricular septum to apex of heart where they turn and run superiorly through outer wall of ventricles • supply papillary muscles before rest of ventricular wall • Why would this be important? Fig. 18.14, p. 691 Fig. 18.17, p. 694
Electrocardiograph (ECG) • Measures electrical changes in heart • Electrocardiograph – instrument used to measure changes • Leads • combinations of electrodes used to detect changes • 12 standard leads • I – right arm (-) -> left arm (+) • II – right arm (-) -> left leg (+) • III – left arm (-) -> left leg (+) • Chest leads http://www.cardioliving.com/consumer/Heart/Electrocardiogram.shtm
Electrocardiogram (ECG) • Electrocardiogram – recording of the changes in membrane potential • Series of deflections from baseline – correspond to spread of action potential through myocardium • Analysis – ECG shows: • overall heart rate • wave shape, height and duration • deviations from normal
Intrinsic Conduction System, pp. 5-6 ECG Waves - Overview • P Wave • PR Interval • QRS complex • QT segment • T wave Fig. 18.16, p. 694
Intrinsic Conduction System, pp. 5-6 ECG : P wave, PR Interval • P wave - depolarization of SA node followed by atrial depolarization • P-R (P-Q) interval • time from beginning of atrial depolarization to onset of ventricular depolarization; • includes spread of AP through atria and conducting system Fig. 18.16, p. 694
ECG Analysis: QRS and T • QRS complex – spread of depolarization through system and both ventricles • Q-T segment – time from onset of ventricular depolarization to end of repolarization • T wave – repolarization of ventricles Fig. 18.16, p. 694 http://www.emergency-nurse.com/resource/clipart/clipart9.htm
Common Cardiac Arrhythmias • Sinus bradycardia – impulses arise at SA node at slower than normal rate (<60 per minute) • Sinus tachycardia – impulses arise at SA node at faster than normal rate (>100 per minute at rest) http://www.rnceus.com/ekg/ekgsb.html http://home.earthlink.net/~avdoc/infocntr/htrhythm/hrstachy.htm