Download
1 / 37
390 likes | 441 Views
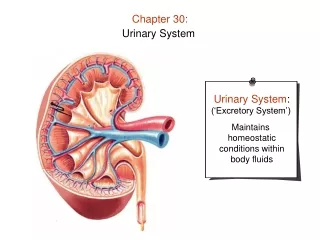
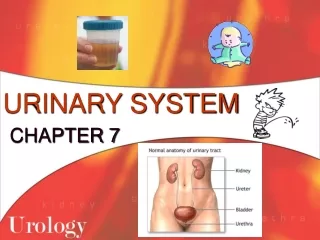
Chapter 89 Urinary Disorders. The Urinary Tract. Upper tract –filters the by-products of metabolism and adjust the body’s fluid and electrolyte balance Kidneys and ureters-damage life threatening Lower tract –acts as a storage area until micturition

E N D
The Urinary Tract • Upper tract –filters the by-products of metabolism and adjust the body’s fluid and electrolyte balance • Kidneys and ureters-damage life threatening • Lower tract –acts as a storage area until micturition • Bladder and urethra-reflux back flow of urine • Urologist –urinary tract • Nephrologist -Kidney • Dialysis nurse
Combining Forms in Urology • cyst(o)- Pertaining to any bladder • lith(o)- Stone • nephr(o)- Pertaining to the kidney • pyel(o)- Pertaining to the renal pelvis • ureter(o)- Pertaining to the ureter • urethr(o)- Pertaining to the urethra • vesic(o)- Usually pertaining to the urinary bladder • -tripsy Crushing
Laboratory Tests • Urinalysis (UA)-Please know chart 1497-urine to lab within 30 minutes • Routine or random UA- special considerations *elderly and the very young-1496 • Nursing considerations for urinalysis • Renal function tests • Blood urea nitrogen (BUN)- determines how efficiently the glomeruli remove the nitrogenous wastes ( urea) that result form protein metabolism :elevated for kidney disease, high protein diet; fluid loss in dehydration • GFR= is ta measurement of the rate of urine formation as blood is filtering thorough the glomeruli of the kidney • Serum creatinine-a product of protein metabolism is related to muscle mas and excreted by the kidney- creatinine is the chief nitrogenous waste of protein metabolism the GFR must be reduced 50 percent before a change is seen in the creatinine and is best indicator for kidney function- usually a basic constant level of measurement • Creatinine clearance test-uses collected urine specimen to indicate glomerular filtration rate and renal insufficiency usually ordered in the morning –best test for early kidney disease-12-24 hour urine collection • Uric acid studies- 24 hour study gouty arthritis or kidney disease
Question Is the following statement true or false? A urinalysis sample need not be refrigerated after being obtained.
Answer False Bacteria in a urinalysis sample will reproduce if the specimen is not refrigerated shortly after being obtained. To prevent false readings, biological specimens (urine, stool, wounds) are processed according to facility protocols.
Imaging Studies • Intravenous pyelogram (IVP)-x-ray films after a radiopaque dye has been injected; check for iodine/shellfish allergy;NPO for 8 hours/laxative the night before; diabetic may have to hold Glucophage for 48 hours and increase water to 2-4 L • Radioactive renogram-shows blood vessels, obstructions; Tumors pick up more radioactive substances than normal tissue • Cystogram and voiding cystourethrogram- x-ray of bladder and urethra by installation of dye directly into the bladder through catheter. Using fluoroscopy-shows reflux
studies • Retrograde pyelogram smaller catheters are introduced into the ureters and then passed into the kidney where dye is injected is combined with the cystoscopy- • Renal arteriogram- injecting contrast through a catheter into the aorta at the level of the renal blood vessels • Endoscopic procedure: Cystoscopy- visualize inside of the bladder-looking for reason for hematuria , opening visual-can cause infections- may also remove polyp- may have hematuria (minimal) after procedure report if last >24 hours • Needle biopsy of the kidney • Following identification of a mass by imaging studies
Urodynamic Tests • Uroflowmetry-noninvasive assessment of the status of micturition –clinets voids in a funneled commode connected to an electronic measuring device • Residual urine volume-bladder empty completely-first a complete emptying of the bladder- usually includes a second void then client is catherized/bladder scanner is also an option=residual greather than 150-200 is considered a significant retention • Cystometrogram (CMG)- • Urethral pressure profile (UPP) • Perineal electromyogram (EMG)
Test • Cystometrogram (CMG)- measurement of bladder pressure during filling –must notify MD/nurse when a sense of fullness is felt*500ml • Urethral pressure profile (UPP)evaluates smooth muscle activity along the urethra • Perineal electromyogram (EMG)-test of the pelvic muscle fucntion
Nursing Process • Data collection • Planning and implementation • General nursing considerations • Postoperative care- please review bullets on 1501 and nursing alert • Evaluation
Question Is the following statement true or false? In case of minor urologic surgical procedures, aggressive client and family teaching is required.
Answer True Because many diagnostic and minor urologic surgical procedures are performed on an outpatient basis, aggressive client and family teaching is required. Clients and families must know how to perform preoperative preparation, and untoward signs to look for after the procedure. This teaching must be carefully documented.
Urinary Incontinence • Refers to involuntary voiding or urine loss- the internal sphincter controls the bladder opening and external the pelvic muscles controls the opening of the urethra below the prostate ( no distinction in women) • Types of incontinence: • Transient (temporary) incontinence-can be reversed with diagnosis and TX-once the cause is found • True or total incontinence-nearly continuous; most common cause removal of prostate see bullets for other causes
Incontinence • Stress incontinence-urinary leakage following a sudden increase in intra-abdominal pressure • Reflex incontinence and urge incontinence-are similar in that both types clients experience urgency before voiding caused by bladder spasm- Reflex caused by bladder instability as a result of upper motor lesion where as urge incontinence is caused by irritation of the bladder wall • Overflow incontinence-when the bladder overfills with urine and is not able to release it because ether the detrusor muscle no longer contracts or blockage
Question Urinary incontinence that happens when the bladder overfills with urine and is not able to release it is referred to as ______________. a. Transient incontinence b. True incontinence c. Stress incontinence d. Reflex incontinence e. Overflow incontinence
Answer e. Overflow incontinence Transient incontinence refers to incontinence that can be reversed with diagnosis and treatment. True or total incontinence is defined as urinary leakage that is nearly continuous. Stress incontinence is urinary leakage following a sudden increase in intra-abdominal pressure. Reflex incontinence is caused by bladder instability as a result of upper motor lesions or neuropathies.
Treatment please review educating client on 1503 and 1504 • Credé’s maneuver-manage overflow-frim gentle pressure above the bladder • Kegel exercises-stress incontinence- increase sphincter tone • Electrical stimulation-pelvic muscle stimulation electrode in the vagina or rectum • Pessary-stress incontinence-device inserted in the vagina 4-8 weeks • Medications-Detrol/ditropan • Surgery-Electrocautery, surgical ureteral reimplantation • Augmentation cystoplasty
Nursing Considerations • Encourage fluids to dilute the urine and to flush irritating substances from the bladder. • Teach the client measures to empty the bladder completely. • Biofeedback and Kegel exercises • Assist the person to manage a urethral or suprapubic catheter.
Urinary Tract Infections • Acute cystitis • Inflammation of the urinary bladder • Chronic cystitis • Recurrent UTI • Acute pyelonephritis • Inflammation of the renal pelvis and medulla • Chronic pyelonephritis • If an acute infection recurs or if an obstruction prevents the passage of urine
Signs of Infection • Dysuria • Frequency • Nocturia • Cloudy urine • Hematuria • Fever, chills, flank pain • Mental status changes (e.g., confusion [elderly])
Inflammatory Disorders • Interstitial cystitis (IC) • Glomerulonephritis • Acute glomerulonephritis • Chronic glomerulonephritis • End-stage renal disease (ESRD)
Obstructive Disorders • Hydronephrosis • Acute hydronephrosis and chronic hydronephrosis • Ureterolithiasis • Bladder stones • Ureter or bladder stones • Ureter stones • Kidney or ureter stones • Kidney stones
Nursing Considerations in Ureterolithiasis • Straining urine for calculi • Caring for the client undergoing stone removal • Client teaching
Ureteral or Urethral Strictures • Fibrous bands can form anywhere along the ureters or the urethra, narrowing it and interfering with urine passage. • The client feels the need to void frequently, but an intense burning sensation accompanies voiding. • Diagnostic studies include • Thorough medical history, urodynamic flow testing • Urethrotomy
Urinary Tract Tumors • Benign renal cysts • Cancer of the kidney (nephroma) • Bladder tumors • Urinary diversions • Urostomy— Ileal conduit urinary diversion and cutaneous ureterostomy • Continent diversions • Continent cutaneous diversion • Neobladder to urethra diversion
Urinary Tract Trauma • Kidney laceration • Bruising of the kidney • Bladder rupture
Changes in Renal Function • Renal impairment • Renal insufficiency • Renal failure (or kidney failure) • Acute renal failure • ESRD
Dialysis • Peritoneal dialysis • Continuous ambulatory peritoneal dialysis (CAPD) • Hemodialysis • Home hemodialysis • Types of shunts • AV fistula or AV graft • Subclavian or jugular IV catheter
Purposes of Dialysis • Remove waste products of protein metabolism from the blood • Remove poisons or toxins from the blood • Remove excess water • Establish or maintain proper levels of electrolytes • Maintain acid–base balance • Instill medications (e.g., antibiotics), electrolytes, or other substances
Question Is the following statement true or false? A person with kidney disease may be short of breath, anemic, or chronically fatigued.
Answer True Healthy kidney produces the hormone erythropoietin, which is necessary for production of red blood cells. A person with kidney disease may be short of breath, anemic, or chronically fatigued because he or she does not have enough hemoglobin molecules to carry oxygen.
Possible Complications of Hemodialysis • Exsanguination • Severe, immediately life-threatening hemorrhage • Septicemia • Air emboli • Hemolytic anemia • Disequilibrium syndrome • Hepatitis
Question Is the following statement true or false? Whenever a client has a cannula placement, he or she should have a single clamp attached to the dressing.
Answer False Cannula separation is a life-threatening emergency. The client can exsanguinate in a matter of minutes. Whenever a client has a cannula placement, he or she should be taught to have two clamps always attached to the dressing, to clamp the ends of the separated cannula quickly until they can be reattached.
Kidney Transplant • Potential cure for the client with renal failure • Proper matching of recipient and donor is crucial. • Rejection of transplanted organs • Complications of antirejection medications