Download
1 / 79
790 likes | 960 Views
The Heart. Functions of the Heart Generate blood pressure Routing blood Ensures one-way blood flow Regulating blood supply. Anatomy of the Heart. Review pages 670 to 676 Pay particular attention to heart chambers and valves. (pg. 675-676). Cardiac Muscle. Similar to skeletal muscle.

E N D
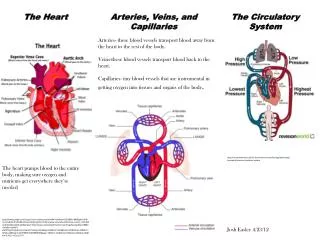
The Heart • Functions of the Heart • Generate blood pressure • Routing blood • Ensures one-way blood flow • Regulating blood supply
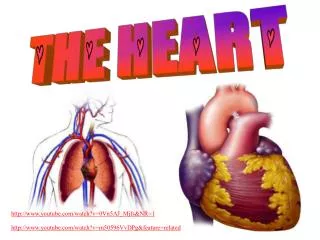
Anatomy of the Heart • Review pages 670 to 676 • Pay particular attention to heart chambers and valves. (pg. 675-676).
Cardiac Muscle • Similar to skeletal muscle. • ATP is used for energy to fuel contraction. • Rich in mitochondria. • Extensive capillary network providing O2.
Cardiac Muscle • Specialized plasma membrane structures called desmosomes hold cells together. • Areas of low resistance between cells called gap junctions allow action potentials to move from one cell to the next.
Conducting System • Two nodes in the cardiac muscle. • Located in the right atrium. • Sinoatrial (SA) node. • Atrioventricular (AV) node. • AV node gives rise to the atrioventricular (AV) bundle. • AV bundle divides to form right and left bundle branches.
Conducting System • Right and left bundle branches terminate in Purkinje fibers. • Cardiac muscle cells have the capacity to generate spontaneous action potentials. • SA node sets the cardiac rhythm (pacemaker).
Conducting System • Once action potentials are initiated at SA node, they spread across the atrium. • The action potentials also travel to the AV node on a pathway that allows a greater velocity. • Therefore, the action potential reaches the AV node before they reach the remainder of the atrium muscle.
Conducting System • At rest, it takes approx. 0.04 second for action potentials to travel from the SA node to the AV node. • Action potentials slow down considerably at the AV node. • It takes 0.11 second for the action potentials to travel through the AV node.
Conducting System • After the action potentials pass through the AV node the conduction velocity increases.
Electrical Properties • Cardiac muscle cells have a resting membrane potential that depends on: • Low permeability to Na+ and Ca2+ • Higher permeability to K+ • When the cardiac muscle cell is depolarized to its threshold, an action potential will result.
Action Potentials • Action potentials in the cardiac muscle are similar to what we discussed earlier. • Cardiac muscle action potentials last longer than those in skeletal muscle.
Action Potentials • Cardiac muscle action potentials have a: • Rapid depolarization phase. • Rapid, partial early repolarization phase. • Prolonged period of slow repolarization (plateau phase). • Rapid final repolarization phase.
Autorhythmicity of Cardiac Muscle • The heart is autorhythmic because it can stimulate itself to contract at regular intervals. • In SA node , pacemaker cells generate action potentials. • These action potentials are generated due to a spontaneous local potential called a prepotential.
Autorhythmicity of Cardiac Muscle • Some cardiac cells can generate their own spontaneous action potential (ectopic focus). • Ectopic foci can result if the: • SA node doesn’t function properly • Blockage of conducting pathways • However, the rhythm set by the SA node is more rapid and produces a heart rate of 70-80 bpm.
Refractory Period • Absolute refractory period • Relative refractory period • Due to the plateau phase and the longer repolarization period, the refractory period is longer.
Electrocardiogram • Action potentials moving through the cardiac muscle produces electrical currents that can be measured on the surface of the body. • These currents are measured by electrodes attached to the surface of the body producing an electrocardiogram (ECG).
Electrocardiogram • The ECG is a diagnostic tool that can be used to determine: • Abnormal heart rates or rhythms • Abnormal conduction pathways • Hypertrophy/atrophy of portions of the heart
Electrocardiogram • Normal ECG consists of a P wave, QRS complex, and a T wave. • The time between the beginning of the P wave and the beginning of the QRS complex is the PR interval. • The time from the beginning of the QRS complex to the end of the T wave is the QT interval.
Arrhythmias • Arrhythmias are abnormal heart rhythms. • Caused when: • the heart’s natural pacemaker develops an abnormal rate or rhythm; • the normal conduction pathway is interrupted; • another part of the heart takes over as the pacemaker.
Arrhythmias • Slow heartbeat (bradycardia) • Can cause fatigue, dizziness, lightheadedness, fainting, or near-fainting spells. • Rapid heartbeat (tachycardia) • Can produce rapid heart action, dizziness, lightheadedness, fainting, or near-fainting spells.
Fibrillation • Atrial fibrillation: • Atria quiver instead of beating correctly. • Blood isn’t pumped out completely. • Blood may pool and form clots which could lodge in the brain and produce a stroke.
Fibrillation • Ventricular fibrillation: • Ventricles contract in a rapid, unsynchronized, uncoordinated fashion. • Little or no blood is pumped from the heart.
Heart Block • The signal from the atria to the ventricles is impaired or isn’t transmitted. • Classified by level of impairment: • First-degree = electrical impulse moves through AV node more slowly than normal(> 0.20 sec). • Second-degree = some signals from atria don’t reach the ventricles (“dropped beats”) • Third-degree = complete AV node block resulting in ventricles setting their own rhythm.
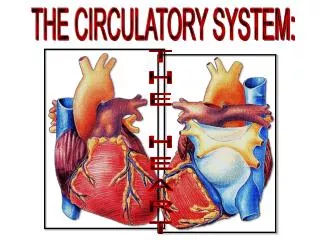
Cardiac Cycle • The heart is actually two pumps; a right half and a left half. • Cardiac cycle refers to the repetitive pumping process that starts with the beginning of one contraction and ends at the beginning of the next contraction. • A normal cardiac cycle lasts 0.7 – 0.8 second.
Cardiac Cycle • Systole = contract • Diastole = dilate (relax) • We will refer to these terms with respect to the ventricles.
Cardiac Cycle • Five phases in the cardiac cycle. • Systole: Isovolumetric ventricular contraction. • Systole: Ventricular ejection. • Diastole: Isovolumetric ventricular relaxation. • Diastole: Passive ventricular filling. • Diastole: Active ventricular filling.
Isovolumetric Ventricular Contraction • Ventricles contract. • Pressure rapidly increases. • All valves remain closed – no blood ejected. • Ventricular volume remains constant.
Ventricular Ejection • Ventricles continue to contract. • Pressure continues to increase. • Pressure in ventricle > pressure in aorta & pulmonary artery (~80 mmHg). • Aortic & pulmonary valves open. • Pressure peaks at ~120 mmHg. • Blood ejection.
Isovolumetric Ventricular Relaxation • Ventricles relax after contraction. • Pressure rapidly decreases. • Aortic & pulmonary valves close. • Volume remains constant.
Passive Ventricular Filling • Atrial pressure exceeds ventricular pressure. • AV valves open. • Blood flows from atria into ventricles. • Accounts for approx. 70% of ventricular filling. • Most filling occurs during first 1/3 of diastole.
Active Ventricular Filling • Depolarization of SA node generates action potentials that spread across atria. • Atria contract during last 1/3 of diastole. • Final volume of blood from atria fills during atrial contraction. • Final volume in ventricle = EDV
Heart Sounds • LUBB-DUPP • LUBB = closure of the AV valves (beginning of systole). • DUPP = closure of the pulmonary & aortic valves.
Mean Arterial Blood Pressure • MAP is the average blood pressure between the systolic and diastolic pressure in the aorta. • MAP Q x PR • Cardiac output (Q) = HR x SV • Stroke volume (SV) is equal to approximately 70 ml. (EDV – ESV).