Download
1 / 19
190 likes | 405 Views
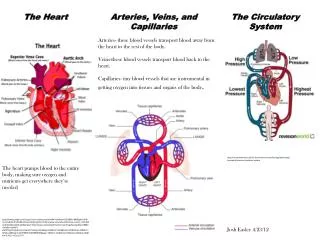
The Heart. THE HEART IS RESPONSIBLE FOR THE CIRCULATION OF THE BLOOD . The heart is actually two pumps in one: 1. one propels blood through the pulmonary circulation (to the lungs where the blood releases carbon dioxide and receives oxygen)

E N D
The Heart • THE HEART IS RESPONSIBLE FOR THE CIRCULATION OF THE BLOOD. • The heart is actually two pumps in one: • 1. one propels blood through the pulmonary circulation (to the lungs where the blood releases carbon dioxide and receives oxygen) • 2. the second propels blood through the systemic circulation (to all remaining tissues of the body).
ANATOMY OF THE HEART • Located in the thoracic cavity between the lungs in a space within the mediastinum called the pericardial cavity • The blunt end of the cone is the apex • The flat top is the base. • The heart is a muscular pump consisting of four chambers: two atria and two ventricles Base Apex
Pericardium • The pericardium or pericardial sac, is a double-layered closed sac that surrounds the heart • fibrous pericardium tough, fibrous connective tissue outer layer prevents over-distention of the heart and anchors the heart in the mediastinum • serous pericardium. a thin, transparent inner layer of simple squamous epithelium • parietal pericardium The portion of the serous pericardium lining the fibrous pericardium • visceral pericardium or epicardium that portion covering the heart surface • (The parietal and visceral portions of the serous pericardium are continuous with each other where the great vessels enter or leave the heart) • pericardial cavity between the visceral and parietal pericardia is filled with a thin layer of serous pericardial fluid that helps reduce friction
Cardiac Muscle • Intercalated disks- has cell to cell special contacts • Desmosomes- hold cells close together • Gap Junctions- low electric Resistance between cells…greater conductivity • Therefore cardiac cells act as a single unit electrically
Conducting System Process • SA Sinoatrial Node- pacemaker of heart (generates action potentials greater frequency) • .04 faster than to surrounding muscle • AV Atrioventricular Node- Slow to transmit action potential and allows completion of atrial contraction • AV Bundle of His • Fast • Bundle branches- right and left • IV Septum • RtVentrical apex • Lt Ventrical apex • Perkinje Fibers- large diameter cardiac muscle • Transmits signal to apex of ventricles • A lot of intercalated disks --- Myocardium in apex contracts in a wringing action
Autorhymicity of Cardiac Muscle • Action potentials in heart without external stimuli • After each action potential the membrane potential returns to its resting membrane potential • Unstable slow ion channels open and cause depolarization • This causes fast channels to open and increase depolarization • When depolarization reaches threshold--action potential happens more often in SA Node because more slow channels • Plateau Phase- Prolonged period of depolarization, separates contractions in the heart • Heart has long action potential so the heart will rest between contractions and not tetanic contractions • Absolute refractory period – CM insensitive to further stimuli
EKG • Electrokardiogram- device to record the action potential of cardiac muscle summation • Cannot detect force of contraction • Cannot detect Blood Pressure • Can detect abnormal heart rates/ rhythems • Can detect abnormal conduction pathways • Can detect hypertrophy and atrophy and relative position of damage • P Wave- Action potential depolarization of atrial myocardium • Causes Atrial contraction • QRS Complex- Ventricular depolarization • Causes onset of ventricular contraction • Also atrial repolarization masked by QRS signal • T Wave- repolarization before ventricular relaxation • PQ/PR Interval- .16 sec- atria contract and relax • QT Interval- .3 sec- ventricles contract and relax • 1 Cardiac Cycle- from onset muscle contraction to next
Heart Sounds • First heart sound • “Lubb”- ventricles contact and both AV valves close • Second heart sound • “Dupp”- semilunar valves close at end of ventricular systole • Systole is between first and second sounds. • Diasole is between second and first sounds.
Blood Pressure • Systolic- to contract • Diastolic- to dialate • Refers to ventricles • 120 systolic / 80 Diastolic Normal 72 beats/min X 70 ml/beat 5040 ml/min=5 L/min Exercise 120 beats/min X 200 ml/beat 24,000 ml/min=24 L/min
Systole • Isometric Contraction – Contraction of the ventricle causes A-V valves to close and pressure to build in heart. • Ejection – Ventricular pressure exceeds the pressure in the pulmonary trunk and aorta and the semilunar valves open to expel the blood. • At around 80mm Hg pressure aortic SLV opens and goes up to 120mm Hg. • At end of systole ventricular volume dropw because the heart runs out of blood.
Diastole • Isometric Relaxations 1.Back flow of blood closes semilunar valves. 2.Pressure drops and AV values open 3.Blood rushes into ventricles from atria. 4.Cardiac Reserve- difference between cardiac output at rest and exercise.
Blood Pressure • Procedure • Center the bladder over the Brachial Artery just medial to the biceps tendon. Apply snugly and securely • Check the palpatory systolic pressure first • Inflate to 20 to 30 mm Hg above the palpatory systolic • Place bell of stethoscope over the brachial artery • Deflate the cuff slowly (2 to 3 mm Hg per sec.) and note the points where the following occurs: • Two consecutive beats are heard typically crisps sounding (indicates systolic pressure)…recorded as auscultatory systolic pressure • A muffling of the pulse sounds recorded as mid-diastolic point. The point at which the sounds begin to fade away. • The sound disappears- (indicates peripheral resistance of arteries)…recorded as end-diastolic pressure.
Ischemia (is-ke'me-ah), - lack of an adequate blood supply to the heart may lead to fibrillation—
MYOCARDIAL INFARCTION • A myocardial infarct is an area of heart tissue in which the cardiac cells have died • it is generally a result of ischemia. • Ischemia (is-ke'me-ah), is lack of an adequate blood supply to the heart
Abnormalities in the shape of the waves and changes in their timing send signals that something may be wrong with the intrinsic conduction system or may indicate a myocardial infarct (present or past).
HEART BLOCK • any damage to the AV node can partially or totally release the ventricles from the control of the SA node. • the ventricles begin to beat at their own rate, which is much slower, some or all of the time • Sn: depolarization waves can reach the ventricles only by traveling through the AV node.
HEART RATE ANOMALIES • Tachycardia is a rapid heart rate (over 100 beats per minute). • Bradycardia is a heart rate that is substantially slower than normal (less than 60 beats per minute). • Neither condition is pathological, but prolonged tachycardia may progress to fibrillation.
FIBRILLATION • fibrillation—a rapid uncoordinated shuddering of the heart muscle • makes the heart totally useless as a pump and is a major cause of death from heart attacks in adults. • During fibrillation, the normal pattern of the ECG is totally lost, and the heart ceases to act as a functioning pump.
Abnormalities in the shape of the waves and changes in their timing send signals that something may be wrong with the intrinsic conduction system or may indicate a myocardial infarct (present or past). • A myocardial infarct is an area of heart tissue in which the cardiac cells have died; it is generally a result of ischemia. • During fibrillation, the normal pattern of the ECG is totally lost, and the heart ceases to act as a functioning pump. • Because the atria and ventricles are separated from one another by "insulating" connective tissue, which is part of the fibrous skeleton of the heart, depolarization waves can reach the ventricles only by traveling through the AV node. Thus, any damage to the AV node can partially or totally release the ventricles from the control of the SA node. When this occurs, the ventricles begin to beat at their own rate, which is much slower, some or all of the time. This condition is called heart block, • damage to the SA node results in a slower heart rate. When this is a problem, artificial pacemakers are usually installed surgically. • Ischemia (is-ke'me-ah), or lack of an adequate blood supply to the heart may lead to fibrillation—a rapid uncoordinated shuddering of the heart muscle makes the heart totally useless as a pump and is a major cause of death from heart attacks in adults. • Tachycardia is a rapid heart rate (over 100 beats per minute). • Bradycardia is a heart rate that is substantially slower than normal (less than 60 beats per minute). • Neither condition is pathological, but prolonged tachycardia may progress to fibrillation.