Download
1 / 19
190 likes | 210 Views
Module: Health Psychology Lecture: Illness Behaviours and Beliefs Date: 02 February 2009. Chris Bridle, PhD, CPsychol Associate Professor (Reader) Warwick Medical School University of Warwick Tel: +44(24) 761 50222 Email: C.Bridle@warwick.ac.uk www.warwick.ac.uk/go/hpsych.

E N D
Module: Health PsychologyLecture: Illness Behaviours and BeliefsDate: 02 February 2009 Chris Bridle, PhD, CPsychol Associate Professor (Reader) Warwick Medical School University of Warwick Tel: +44(24) 761 50222 Email: C.Bridle@warwick.ac.ukwww.warwick.ac.uk/go/hpsych
Aims and Objectives • Aim: To provide an overview of the psychological determinants of illness-related behaviours and beliefs • Objectives: To enable students to begin formulating answers to the following questions: • Which psychological factors influence symptom perception and symptom reporting? • Why do some people consistently report more / fewer symptoms than others? • Why do some people delay seeking medical help, while others are quick to the doctor for minor complaints? • What types of belief do people hold in order to understand their illness?
Definitions • Illness behaviour: Any response directed by perceptions of illness: objective or subjective; confirmed or suspected, self or other notified, e.g. help seeking, treatment adherence, behaviour change, etc. • Illness beliefs: A patient’s implicit understanding of their health status based on common-sense beliefs about their illness, e.g. beliefs about the cause, course and consequences of the illness • Illness representations: Clustering of related beliefs along dimensions to form an explicit understanding, or picture, of illness that serves to direct coping responses and illness behaviour
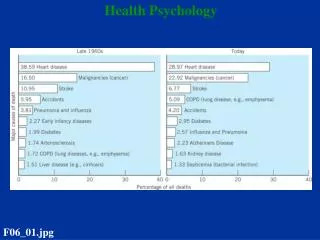
Symptom Prevalence • How prevalent are physical symptoms in a UK general population? • Over 1-week, 69%/1410 adults reported experiencing at least one physical symptom: • Headache (38%); Sleep disturbance (32%); aching bones, joints and muscles (29%); skin and eye problems (27%). • About 90% of symptom experiences are not accompanied by seeking medical help. (Koenke, 2003)
Symptom Perception and Reporting • Which psychological factors influence whether people notice physical symptoms and respond to symptom perception? • Where can you start? • Module framework: • Background • Stable • Social • Situational
Background Influences • Social knowledge and beliefs about illness and help seeking • Ethnicity; Gender; SES; Culture; Media; etc. • Health status: People with chronic conditions report more and fewer symptoms … … … … urgh? • Over-reporting of symptoms that relate to the condition • Under-reporting of symptoms that (they believe) are unrelated to condition
Stable InfluencesIn what way do stable factors influence symptom perception & reporting? • Emotional disposition • Ps with negative affect are more likely to notice symptoms, report more symptoms and do so more quickly, i.e. high false-positive • Ps with low expression block emotionally arousing stimuli and tend to report fewer symptoms, i.e. high false-negative • Generalised expectancies (future positive outcome) • Ps with favourable outcome expectancies (I-LoC; high Self-efficacy) report fewer symptoms ... But there might be a cost … • Lack of vigilance + control beliefs = delay & disease progression • Explanatory style (current negative outcome) • Pessimistic styles perceive more symptoms and symptoms of greater severity, but delay help seeking • Internalising style increases vigilance of self and the tendency to report more symptoms, more quickly.
Social InfluencesWhat social factors influence symptom perception & reporting? • Illness information often from social cues • ‘You look a bit pale’ – cues a search for confirmatory evidence • Lay referral network for advice, diagnosis and treatment • Being a medical student • Symptom information leads to symptom searching; easier to confirm presence rather than confirm absence; • Report more symptoms but seek less help! • Perceived social support • High: rate oneself as more healthy, recall fewer illness-related memories, and report fewer symptoms • Low: higher perceived vulnerability to illness, pessimistic about symptom relief, and report more symptoms
Situational InfluencesWhat situational factors influence symptom perception & reporting? • Competition for cues (attention) • More attentive to symptoms when situation is boring • H = frequency of coughing inversely related to excitement of lecture • Stress (acute) • Often precipitate and/or aggravate perception and reporting of physical symptoms • Increases perceived vulnerability to illness, and/or mis-attribution of physiological reactivity as symptoms of illness • Symptom characteristics • Onset speed; Public visibility; Causal specificity; Chronic illness-related complication • High emotional response to symptom recognition can speed help seeking, but delay if too high, e.g. emotional suppression
Illness Representations • Illness beliefs refer to a patient’s own implicit common-sense understanding of their illness • Patients may have numerous beliefs for a particular illness • Five belief dimensions: • Identity:what is it? • Cause:what caused it? • Time:how long will it last? • Consequence:how will it impact my life? • Control-Cure:can it be treated, controlled, managed, etc? • Dimensions form the patient’s illness representation • Illness representations direct illness behaviours
Identity • Identity refers to the (diagnostic) label patients give to their illness • Illness label (i.e. identity) is based on beliefs about the symptoms of the illness • Illness beliefs may be incorrect and / or unhelpful • Labels bias the salience, interpretation and assimilation of illness-related information • Increased salience of label-relevant information, i.e. attentional bias • Interpret new information (e.g. symptoms) in light of dominant illness representation • Assimilate new information if consistent with current beliefs, i.e. reject inconsistent / disconfirming information
Cause • Patients develop ideas about the cause of their illness • Genetic; Lifestyle; Stress; Environmental; Chance; etc. • Causal beliefs influence treatment expectations: • Type, e.g. homeopathic or medical, pharmacological or psychological, intervention or watchful waiting, etc. • Adherence to treatment and advice influenced by degree of consistency with expectations • Causal beliefs influence emotional response to illness: • Cancer self-blame; STIs anger; Genetic conditions guilt and helplessness • Intensity of emotional response is a prognostic marker with both direct and indirect pathways of influence
Time • Three main timelines for illness • Acute (e.g. flu); Chronic (e.g. heart disease); Cyclical (e.g. hay fever) • Mismatch in perceived time and natural illness course is not uncommon • Hypertension commonly believed to be cyclical, e.g. high blood pressure only when stressed • Negates the need to take medication
Consequences • Perceived effect of illness on the patient’s life • Personal identity, social relationships, finances, etc. • Perceived severity of consequences is prognostic • After controlling for clinical factors, MI patients who perceived consequence as more severe on admission • Had longer hospital stay (md = 4 days) and, after discharge, took longer to return to work (md = 4 months) • Reported greater disability and increased psychological morbidity at 1 year • Had a 60% increased risk for cardiovascular-related morbidity and mortality at 2 years (Petrie et al., 2003)
Control-Cure • Beliefs about how an illness can be treated and the effectiveness of treatment • Patients who believe its possible to control illness are more likely to • Adapt to the consequences of the illness • Attend rehabilitation programmes • Adhere to treatment
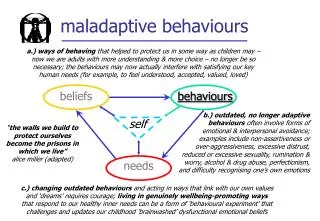
Conclusions • Psychological processes influence recognition of symptoms (perception), understanding of illness (beliefs) and response to illness (behaviour) • Illness beliefs cluster together to form a patient’s representation of their illness • Identity; Cause; Time; Consequences; Cure-Control • Inappropriate illness behaviours will often reflect maladaptive illness representations / distorted illness beliefs • Asking patients open-ended questions about their thoughts and ideas about their illness is a simple way to • Bring the biopsychosocial model into clinical practice • Identify and address minor, but maladaptive, misconceptions
Summary • This session would have helped the student to understand the … • range of behaviours that can be described as being illness behaviours • types of illness beliefs that help patients form an understanding / representation of their illness • how illness representations shape behavioural responses to perceived illness • psychological factors that explain variation in patient responses to illness
Next Week • Consultation • Patients attend consultation with fairly well-developed illness representations and resultant expectations • Differing representations and expectations (patient & Dr) make consultation difficult and unsatisfactory • Unsatisfactory consultations undermine treatment effectiveness … … … … and you’ve not even met your patient yet!
Any questions? • What now? • Obtain / download one of the recommended readings • Consider today’s lecture in relation to your tutorial • Your tutorial begins at 3.15