Download
1 / 72
720 likes | 887 Views
This presentation by Dr. Anna L. Marsland discusses the intricate relationships between the central nervous system (CNS) and the immune system, highlighting their implications for health and disease. Drawing on the biopsychosocial model and principles of psychoneuroimmunology, the talk covers various pathways, including anatomical and neurochemical links that influence immune function. It examines how stress and affective states impact cellular immunity and explores mechanisms behind individual variations in immune reactivity. The research methods and findings underscore the importance of understanding these interactions for managing health outcomes.

E N D
Bidirectional Pathways between the Central Nervous and Immune Systems: Implications for Disease Anna L. Marsland, Ph.D., RN Behavioral Immunology Laboratory University of Pittsburgh
Psychoneuroimmunology Study of interrelations between the central nervous and immune systems and their implications for health
Pathways between the CNS and Immune Systems (Sternberg, 2006 Nature Reviews Immunology, 6, 318-28)
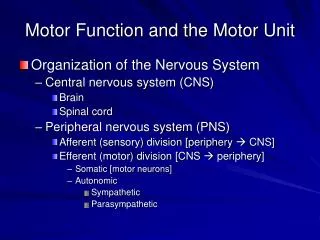
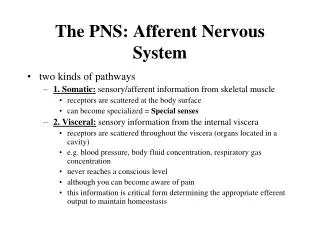
Evidence for Pathways Between the CNS and Immunity • Anatomical links between the nervous and immune systems • Autonomic innervation of immune organs (e.g., Felten et al., 1992. Chem. Immunol 52, 25-48) • Receptors on immune cells for neurochemicals released in response to emotions (e.g., Sanders & Kohm, 2002 Int. rev Neurobiol 53, 17-41) • Consistent evidence for neuroendocrine-induced alteration of specific immune functions (e.g., Elenkov et al., 1996 Proc assoc Am Physicians 108:374-381)
Outline of Talk Dispositional Affect Stress BRAIN Systemic cytokines Parasympathetic Nervous System Sympathetic Nervous System 3 Activated Immune Cells 1 2 IMMUNE SYSTEM Cellular Immunity Inflammation Antigen
1 Stress and Cellular Immunity
LIFE EVENT STRESS Job stress Unemployment Death of loved one Caring for relative with dementia Divorce Marital conflict Natural disasters.. IMMUNE COVARIATES NK cell activity lymphocyte proliferation Activity latent viruses e.g., herpes Human Studies Segerstrom & Miller, 2004. Psych Bull 130,601-30
Acute Stress / Daily Hassles Does acute stress also influence cellular immune functioning in healthy individuals? • Permit causal interpretations • Allow control for extraneous factors • A means to investigate physiological pathways • Provide model for transient daily life stressors
Does acute laboratory stress alter cellular immune components? • What are the mechanisms of stress-induced changes in immunity? • Are individual differences in the magnitude of immune reactivity stable across time? • Are individual differences in stress-induced immune reactivity related to ability to resist infection?
Protocol Minutes 0 5 10 15 20 25 30 35 40 45 50 * * Baseline Task * - HR and BP taken every 90 seconds
Measures of Cellular Immunity Assessment of the numbers of various subgroups of immune cells.
Measure of Cellular Immune Function: Lymphocyte Proliferation Mitogen Suspension Tritiated Thymidine lymphocytes Culture Medium Filter Measure radioactivity centrifuged whole blood
Does acute laboratory stress alter cellular immune components? • What are the mechanisms of stress-induced changes in immunity? • Are individual differences in the magnitude of immune reactivity stable across time? • Are individual differences in stress-induced immune reactivity related to ability to resist infection?
Stress-Related Increases in Numbers of Circulating NK and Cytotoxic T Cells P’s < .005 Marsland et al., 2002. Physiology and Behavior, 77, 711-16
Proliferative Responses during the Stroop Test Herbert et al., 1994; Psychosom Med 56, 337-44
Does acute laboratory stress alter cellular immunecomponents? • What are the mechanisms of stress-induced changes in immunity? • Are individual differences in the magnitude of immune reactivity stable across time? • Are individual differences in stress-induced immune reactivity related to ability to resist infection?
Hemoconcentration Small blood vessel Increased blood pressure
Changes in Plasma Volume From Before to After Stress All significant, p < .001 Marsland et al., 1997, Health Psychol 16, 1-8.
Changes in Number of Helper-T Cells Before and After Adjustment for Hemoconcentration All significant, p < .001 Marsland et al., 1997, Health Psychol 16, 1-8.
Changes in Number of B Cells Before and After Adjustment for Hemoconcentration All significant, p < .001 Marsland et al., 1997, Health Psychol 16, 1-8.
Possible Active Mechanisms: The Sympathetic Nervous System Individuals differ in the magnitude of their sympathetic responses to acute laboratory challenge, does immunologic reactivity parallel this variability?
PHA Proliferation Response Baseline Task Marsland et al., 2002. Physiology and Behavior, 77, 711-16
PHA Response to Stress With and Without Labetolol Bachen et al., 1995, Psychosom Med 57, 673-9.
Does acute laboratory stress alter cellular immunecomponents? • What are the mechanisms of stress-induced changes in immunity? • Are individual differences in the magnitude of immune reactivity stable across time? • Are individual differences in stress-induced immune reactivity related to ability to resist infection?
Test-Retest Correlations of Residualized Change Scores across time*p<.05; **p<.005 Marsland et al., 1995, Psychosom Med 57, 1163-7
Test-Retest Correlations of Residualized Change Scores across task**p<.005, ***p<.0005 Marsland et al., 2002 Psychophysiology, 39:865-868.
Does acute laboratory stress alter cellular immunecomponents? • What are the mechanisms of stress-induced changes in immunity? • Are individual differences in the magnitude of immune reactivity stable across time? • Are individual differences in stress-induced immune reactivity related to ability to resist infection?
Hepatitis B Vaccination Model • In vivo antibody response to novel antigen Participants • 84 healthy graduate students • 51 male • Aged 21-33 (mean = 24)
Protocol MONTHS *10ml blood draw to determine antibody response to hepatitis B surface antigen 0 1 2 3 4 5 6 7 8 9 10 T2 Ab* T1 Ab*
Baseline and Weight-Adjusted Change in PHA 10 ug/ml Low A High A p < .03 Marsland et al., 2001 Health Psychol 20: 4-11
Positive and Negative Affect among High and Low in Antibody Responders Low Ab High Ab Marsland et al., 2006, Brain, Behav Immun, 20:261-269
Conclusions 1 • Acute stress is associated with a down regulation of cellular immune function mediated by activation of the sympathetic nervous system • Individuals vary markedly in the magnitude of this immune response and this variability is relatively stable across time and task • Individual differences in the magnitude of this immune reactivity may form a physiologic basis for differences in susceptibility to infection at times of naturalistic stress.
Outline of Talk Dispositional Affect Acute Stress BRAIN Parasympathetic Nervous System 2 Innate Immunity Antigen
Chronic systemic inflammation Cardiovascular disease Diabetes Arthritis General functional decline Alzheimer’s disease
Macrophage-Derived Pro-Inflammatory Mediators Activated macrophages Cytokines Chemokines TNF-alpha IL-6 IL-1beta IL-8 Recruit and activate leukocytes from circulation Attracts neutrophils and naïve T cells
Proinflammatory Mediators and Disease • Circulating levels of proinflammatory cytokines predict future inflammatory disease • Cardiovascular disease risk in healthy subjects (e.g., Ridker et al., 2000, Circulation 342,836-.) • Exacerbation of autoimmune diseases (Papanicoloaou et al., 1998, Ann Intern Med 128, 127.)
Psychosocial Risk Factors for Inflammatory Disease Psychosocial Risk Factors Depressive Symptoms Trait Negative Affect Psychological Stress Hostility Cardiovascular Disease Multiple Sclerosis Rheumatoid Arthritis Psoriasis Type 2 diabetes
Are psychosocial risk factors for inflammatory disease associated with systemic inflammation?
Common Factor: Trait Negative Affect Trait Negative Affect
Associations between Antagonistic Dispositions and Inflammatory Markers (n = 855; 31-54 years) * p<.05; **p<.005
Relationships between Hostility Dimensions and IL-6 Hostile Cognitions β =.07, p =.05 Negative Affect Hostile Affect IL-6 β = .06, p = .06 β=.10, p =.007 Hostile Behavior β = .12, p =.002 β= .09, p =.04 Covariates: age, sex, race, years of education, and hypertension
Relationships between Hostility Dimensions and CRP Hostile Cognitions β =.11, p =.002 Negative Affect Hostile Affect CRP β = .07, p = .03 β=.09, p =.009 Hostile Behavior β= .08, p =.04 β = .11, p =.003 Covariates: age, sex, race, years of education, and hypertension
Antagonistic Behavior and Systemic Inflammation (N = 855) Marsland et al., in press, Brain, Behavior and Immunity