Download
1 / 1
10 likes | 179 Views
2-3 rpts. 10 rpts. 2 rpts. 12 rpts. 10 rpts. 21 rpts. 11 rpts. 4 rpts. 10 rpts. 21 rpts. 2-3 rpts. Expansion Positive. Sizing PCR:. RP-PCR:. C9orf72:. gDNA. NM_145005.4. NM_018325.2. N. E1. E2. 23.1kb. 9.4kb. 6.6kb. R2. Sizing PCR. R1. R2. R1. RP-PCR. (GGGGCC)n.

E N D
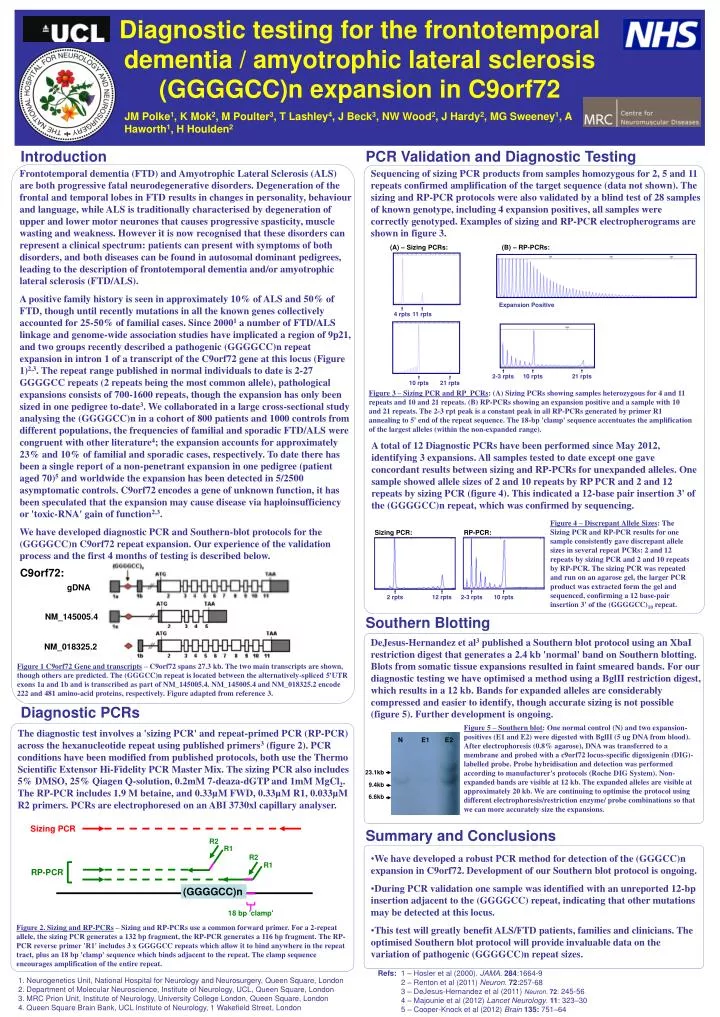
2-3 rpts 10 rpts 2 rpts 12 rpts 10 rpts 21 rpts 11 rpts 4 rpts 10 rpts 21 rpts 2-3 rpts Expansion Positive Sizing PCR: RP-PCR: C9orf72: gDNA NM_145005.4 NM_018325.2 N E1 E2 23.1kb 9.4kb 6.6kb R2 Sizing PCR R1 R2 R1 RP-PCR (GGGGCC)n 18 bp 'clamp' Diagnostic testing for the frontotemporal dementia / amyotrophic lateral sclerosis (GGGGCC)n expansion in C9orf72 JM Polke1, K Mok2, M Poulter3, T Lashley4, J Beck3, NW Wood2, J Hardy2, MG Sweeney1, A Haworth1, H Houlden2 Introduction PCR Validation and Diagnostic Testing Frontotemporal dementia (FTD) and Amyotrophic Lateral Sclerosis (ALS) are both progressive fatal neurodegenerative disorders. Degeneration of the frontal and temporal lobes in FTD results in changes in personality, behaviour and language, while ALS is traditionally characterised by degeneration of upper and lower motor neurones that causes progressive spasticity, muscle wasting and weakness. However it is now recognised that these disorders can represent a clinical spectrum: patients can present with symptoms of both disorders, and both diseases can be found in autosomal dominant pedigrees, leading to the description of frontotemporal dementia and/or amyotrophic lateral sclerosis (FTD/ALS). A positive family history is seen in approximately 10% of ALS and 50% of FTD, though until recently mutations in all the known genes collectively accounted for 25-50% of familial cases. Since 20001 a number of FTD/ALS linkage and genome-wide association studies have implicated a region of 9p21, and two groups recently described a pathogenic (GGGGCC)n repeat expansion in intron 1 of a transcript of the C9orf72 gene at this locus (Figure 1)2,3. The repeat range published in normal individuals to date is 2-27 GGGGCC repeats (2 repeats being the most common allele), pathological expansions consists of 700-1600 repeats, though the expansion has only been sized in one pedigree to-date3. We collaborated in a large cross-sectional study analysing the (GGGGCC)n in a cohort of 800 patients and 1000 controls from different populations, the frequencies of familial and sporadic FTD/ALS were congruent with other literature4; the expansion accounts for approximately 23% and 10% of familial and sporadic cases, respectively. To date there has been a single report of a non-penetrant expansion in one pedigree (patient aged 70)5 and worldwide the expansion has been detected in 5/2500 asymptomatic controls. C9orf72 encodes a gene of unknown function, it has been speculated that the expansion may cause disease via haploinsufficiency or 'toxic-RNA' gain of function2,3. We have developed diagnostic PCR and Southern-blot protocols for the (GGGGCC)n C9orf72 repeat expansion. Our experience of the validation process and the first 4 months of testing is described below. Sequencing of sizing PCR products from samples homozygous for 2, 5 and 11 repeats confirmed amplification of the target sequence (data not shown). The sizing and RP-PCR protocols were also validated by a blind test of 28 samples of known genotype, including 4 expansion positives, all samples were correctly genotyped. Examples of sizing and RP-PCR electropherograms are shown in figure 3. (A) – Sizing PCRs: (B) – RP-PCRs: Figure 3 – Sizing PCR and RP_PCRs: (A) Sizing PCRs showing samples heterozygous for 4 and 11 repeats and 10 and 21 repeats. (B) RP-PCRs showing an expansion positive and a sample with 10 and 21 repeats. The 2-3 rpt peak is a constant peak in all RP-PCRs generated by primer R1 annealing to 5' end of the repeat sequence. The 18-bp 'clamp' sequence accentuates the amplification of the largest alleles (within the non-expanded range). A total of 12 Diagnostic PCRs have been performed since May 2012, identifying 3 expansions. All samples tested to date except one gave concordant results between sizing and RP-PCRs for unexpanded alleles. One sample showed allele sizes of 2 and 10 repeats by RP PCR and 2 and 12 repeats by sizing PCR (figure 4). This indicated a 12-base pair insertion 3' of the (GGGGCC)n repeat, which was confirmed by sequencing. Figure 4 – Discrepant Allele Sizes: The Sizing PCR and RP-PCR results for one sample consistently gave discrepant allele sizes in several repeat PCRs: 2 and 12 repeats by sizing PCR and 2 and 10 repeats by RP-PCR. The sizing PCR was repeated and run on an agarose gel, the larger PCR product was extracted form the gel and sequenced, confirming a 12 base-pair insertion 3' of the (GGGGCC)10 repeat. Southern Blotting DeJesus-Hernandez et al3 published a Southern blot protocol using an XbaI restriction digest that generates a 2.4 kb 'normal' band on Southern blotting. Blots from somatic tissue expansions resulted in faint smeared bands. For our diagnostic testing we have optimised a method using a BglII restriction digest, which results in a 12 kb. Bands for expanded alleles are considerably compressed and easier to identify, though accurate sizing is not possible (figure 5). Further development is ongoing. Figure 1 C9orf72 Gene and transcripts – C9orf72 spans 27.3 kb. The two main transcripts are shown, though others are predicted. The (GGGCC)n repeat is located between the alternatively-spliced 5'UTR exons 1a and 1b and is transcribed as part of NM_145005.4. NM_145005.4 and NM_018325.2 encode 222 and 481 amino-acid proteins, respectively. Figure adapted from reference 3. Diagnostic PCRs Figure 5 – Southern blot: One normal control (N) and two expansion-positives (E1 and E2) were digested with BglII (5 ug DNA from blood). After electrophoresis (0.8% agarose), DNA was transferred to a membrane and probed with a c9orf72 locus-specific digoxigenin (DIG)-labelled probe. Probe hybridisation and detection was performed according to manufacturer's protocols (Roche DIG System). Non-expanded bands are visible at 12 kb. The expanded alleles are visible at approximately 20 kb. We are continuing to optimise the protocol using different electrophoresis/restriction enzyme/ probe combinations so that we can more accurately size the expansions. The diagnostic test involves a 'sizing PCR' and repeat-primed PCR (RP-PCR) across the hexanucleotide repeat using published primers3(figure 2). PCR conditions have been modified from published protocols, both use the Thermo Scientific Extensor Hi-Fidelity PCR Master Mix. The sizing PCR also includes 5% DMSO, 25% Qiagen Q-solution, 0.2mM 7-deaza-dGTP and 1mM MgCl2. The RP-PCR includes 1.9 M betaine, and 0.33µM FWD, 0.33µM R1, 0.033µM R2 primers. PCRs are electrophoresed on an ABI 3730xl capillary analyser. Summary and Conclusions • We have developed a robust PCR method for detection of the (GGGCC)n expansion in C9orf72. Development of our Southern blot protocol is ongoing. • During PCR validation one sample was identified with an unreported 12-bp insertion adjacent to the (GGGGCC) repeat, indicating that other mutations may be detected at this locus. • This test will greatly benefit ALS/FTD patients, families and clinicians. The optimised Southern blot protocol will provide invaluable data on the variation of pathogenic (GGGGCC)n repeat sizes. Figure 2. Sizing and RP-PCRs – Sizing and RP-PCRs use a common forward primer. For a 2-repeat allele, the sizing PCR generates a 132 bp fragment, the RP-PCR generates a 116 bp fragment. The RP-PCR reverse primer 'R1' includes 3 x GGGGCC repeats which allow it to bind anywhere in the repeat tract, plus an 18 bp 'clamp' sequence which binds adjacent to the repeat. The clamp sequence encourages amplification of the entire repeat. Refs: 1 – Hosler et al (2000). JAMA.284:1664-9 2 – Renton et al (2011) Neuron. 72:257-68 3 – DeJesus-Hernandez et al (2011) Neuron. 72: 245-56 4 – Majounie et al (2012) Lancet Neurology. 11: 323–30 5 – Cooper-Knock et al (2012) Brain135: 751–64 • Neurogenetics Unit, National Hospital for Neurology and Neurosurgery, Queen Square, London • Department of Molecular Neuroscience, Institute of Neurology, UCL, Queen Square, London • MRC Prion Unit, Institute of Neurology, University College London, Queen Square, London • Queen Square Brain Bank, UCL Institute of Neurology, 1 Wakefield Street, London