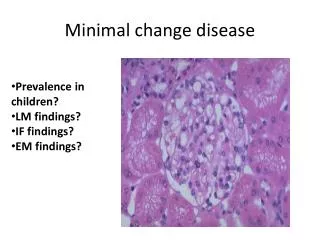
Download
1 / 23
230 likes | 330 Views
Learn about the principles and applications of minimal residual disease (MRD) monitoring in acute myeloid leukemia (AML), including molecular techniques like PCR and flow cytometry. Understand the importance of early detection for guiding treatment decisions and predicting relapse.

E N D
Monitoring of Minimal Residual Disease Principles and Applications Pei Lin, MD Department of Hematopathology UT M.D. Anderson Cancer Center, Houston, TX
MRD studies in AML: Potential Utility • Definition: Residual disease morphologic complete remission (CR) (≤ 5% blasts) • Time points of testing: post induction, post consolidation, pre-transplant, during CR • Prognostic in most studies • Effectiveness of therapy: quantitative, kinetics • Guidance for risk adjusted therapy • Distinguish early recovery from persistent AML • Predicting early relapse
Methods MRD by PCR Leukemic fusion genes (PML-RARA) Mutations (NPM1) Gene overexpression (WT1) Multiparameter flow cytometry (FCM)
Translocation-specific Quantitative RT-PCR Break-Point Reverse Primer Forward Primer Fluorescent Taqman Probe Amplicon t(8;21) RUNX1-RUNX1T1 Positive Negative
MRD by PCR: Leukemic Fusion Transcripts • Recurrent fusions, e.g. t(15;17), t(8;21), inv(16) • Together ~30% of AMLs • qRT-PCR assays • Highly sensitive (1 in 105-106) • Normalize to control • Absolute copy number vs. degree of reduction • RNA instability, turn around time • Limited applicability • Establish standardized assays and cut-offs
Mutation detection – NPM1 Std. RT-PCR wild type mutated • NPM1 mutations in ~30% of overall AML, ~50% of AML with normal karyotype • Most are 4 bp insertions, two adjacent sites • Allele-specific primers detect 1 in 104-105 • Post-therapy MRD is prognostic, can monitor kinetics to predict relapse* • Other potential markers: FLT3, MLL-PTD, KIT, DMNT3A *Schnittger et al. 2009, Blood 114:2220
Detection of MRD by flow cytometry in AML • Identify aberrant vs. normal myeloid precursors • Leukemia-associated immunophenotypes [LA(I)Ps]: • Aberrant lymphoid antigen (CD19, CD7, CD56…) • Aberrant levels of normally expressed antigens (↓,↑ CD38, CD34…) • Coexpression of early and later antigens (CD34++CD15++) • Altered forward and side scatter
Approaches • Must know the patterns of normal and recovering bone marrow • If available, compare MRD to the original phenotype • Need detailed description of antigen expression or dot-plots • Rely on “LAIP” or deviation form normal to identify leukemic cells
Criteria for Dx and Sensitivity • LAIP vs “different-from normal” approach • A: LAIP approach: • Find aberrant clusters of at least 20 cells, showing abnormal expression of at least 2 markers in the LAIP box • Many “LAIP” have a low frequency in normal BM • B: “different-from normal” approach (monocytic leukemia)
8-color MRD: Baseline study Courtesy of Dr. Jeffrey Jorgensen
BM CD34+: Normal vs. AML MRD Normal AML MRD, 0.1% Courtesy of Dr. Jeffrey Jorgensen
Patient 1 FG, 1-31-2013 FG, 11-9-2012 CD117PE Normal CD34 PE-CY7
Patient 2: 21 days post induction Morphology: 21% of blasts
Post therapy CD34 PE-Cy7 CD64 APC Original
Sensitivity To yield sensitivity of 0.01%, collect at least 200K cells per tube (20/200K = 1 in 104 = 0.01%) Sensitivity may be limited due to background normal cells, 0.1% or higher * 0.1% is commonly used threshold in the literature
Detection of MRD by Flow Cytometry • Advantages: • Widely applicable (90- 95% of cases) • Relatively rapid turn around time • Disadvantages: • Interpretation often challenging, requires experience • Can be expensive • Lack of standardization
Potential challenges • LAIPs may not cover all leukemic blasts, partial overlap with normal • Antigen shift resulting from selection/emergence of subclones • A complete change in LAIPs in about 20% of AML, with 80% having at least one LAIP similar to the original (Voskova et al) • Post therapy hypocellular sample • Use a comprehensive panel of antibodies to establish baseline
Summary • MRD detection by FCM or/and PCR are promising tools to guide therapy and to improve outcomes • Each method has pros and cons • More studies are underway to better incorporate the data into clinical decision making (dose intensification and/or ASCT) • Timing of MRD testing by FCM and the cut off levels for each time point that are significant are being refined
Acknowledgement • Dr. Jeffrey Jorgensen MD Anderson Cancer Center