Download
1 / 84
920 likes | 1.53k Views
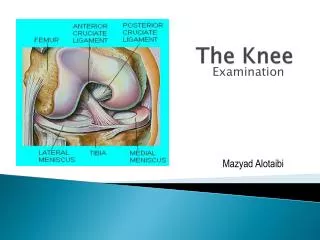
Osteotomies about the Knee. Geoffrey F Dervin, MD, MSc Associate Professor Chairman, Division of Orthopaedic Surgery University of Ottawa. Outline. General indications Technical issues Associated ligamentous deficiencies complications. Symptomatic medial OA. UNI ? HTO ? TKR ?

E N D
Osteotomiesabout the Knee Geoffrey F Dervin, MD, MSc Associate Professor Chairman, Division of Orthopaedic Surgery University of Ottawa
Outline • General indications • Technical issues • Associated ligamentous deficiencies • complications
Symptomatic medial OA • UNI ? • HTO ? • TKR ? • How to decide ? • Who to decide ? Surgeon or patient
B.S. 50 yo active male tennis playerDisabling medial pain After partial resection Degenerative medial Meniscal tear ….but 3 months post scope - still very symptomatic
Indications Best patient: • Moderate OA …Grade 3 or focal area of grade 4 kissing lesion • ROM 10 – 100 minimum • Not obese • Active ….physiologically young – sportive • Non smoker
Major determinants in deciding whether to offer HTO for medial OA : 1. Patient needs , expectations 2. Patient age 3. Disease severity 4. Patient preference
Indications • Best patient…..rarely exists • Compromise some indications if younger, i.e. accept worse severity • Act as a bridge to total knee replacement
Issues in selection: Patient expectations Compliance with rehab a concern ? • Lean to UNI • Pain relief needed • Expect a little less with HTO • ADLs wishes….sports.. • Permit a little more with HTO
Issues in selection: Age !Life Remaining 35 40 50 60 70 80 85 18 years 23 years 32 years 40 years Courtesy J Rudan
Goals of osteotomy: 1.Correction of coronal alignment • Some discretion based on OA severity • More extensive the bone loss – more lateral desired mechanical WBL
Goals of osteotomy: 2.Correction of sagittal alignment Tibial slope
Posterior Tibial Slope 1.Take midpoint of lateral tibia at 10 and 20 cm inferior to tibial plateau 2. Draw perpendicular line 3. Trace line along posterior plateau 4. Measure angle subtended between lines 10cm & 20 cm
Posterior Tibial Slope Normative Data - Sagittal Plane Study Slope Angle Lecuire, 1980 6 ° Bonnin, 1990 10 + 3.1° Paley, 1992 10 ° Insall, 1993 10 ° Dejour, 1994 10 + 3.1° Paley, 1994 9 + 3° 10cm & 20 cm
Tibial vs. Meniscal SlopeJenny JY et al Rev Chirurg Orthop 1997, 83; 435-438. • Posterior horn of menisci thicker • Bony slope mean 84.4º± 2.9 SD • Meniscal slope 90.5º ± 4.1 SD 10°± 2° Meniscal slope Bony slope
Sagittal wear patterns in OA of kneeAnteromedial osteoarthritis of the knee White, Ludkowski, Goodfellow JBJS 73 B(4): 1991 • Medial compartment arthrosis – 46 specimens • ACL intact • Deepest erosion anterior to midpoint • Posterior tibial plateau consistently spared
Sagittal wear patterns in OA of ACL intact kneeAnteromedial osteoarthritis of the knee White, Ludkowski, Goodfellow JBJS 73 B(4): 1991 • Medial compartment arthrosis – 46 specimens • ACL intact • Deepest erosion anterior to midpoint • Posterior tibial plateau consistently spared Posterior Anterior
Sagittal wear patterns in OA of ACL intact knee Posterior Lateral Medial Anterior Anteromedial OA
Sagittal wear patterns in OA of knee – standard anteromedial ( excessive)
Sagittal wear patterns in OA of knee – standard anteromedial ( excessive)
Development of degenerative “cupula”
Sagittal wear patterns in OA of knee – ACL deficient - posteromedial Anterior subluxation… Posterior wear
Sagittal wear patterns in OA of knee – ACL deficient - posteromedial Posterior
Contributors to AP Knee Stability: • Cruciate Ligaments • Menisci • Joint Capsule • Tibial slope
Radiographic Evaluation in isolated ACL RUPTURE (281 cases): Bonnin 1994
Surgically should aim to adjust sagittal slope according to patient characteristics • Ligamentous intact knee • ACL deficient knee • PCL deficient knee
Effects of Increasing Tibial Slope onthe Biomechanics of the KneeJ. Robert Giffin, MD, Tracy M. Vogrin, MS, Thore Zantop, Savio L-Y. Woo, PhD, DSc, andChristopher D. Harner,* MD • The American Journal of Sports Medicine, Vol. 32, No. 2; 376-82: 2004.
Effects of Increasing Tibial Slope onthe Biomechanics of the Knee • The American Journal of Sports Medicine, Vol. 32, No. 2; 376-82: 2004. • Total AP laxity & in-situ forces unchanged • at the new anterior resting position
The American Journal of Sports Medicine, Vol. 32, No. 2; 376-82: 2004.
Deflexion (Extension) Osteotomy Dejour 1994 With ACL DEFICIENT KNEE • First described by Slocum (1983) • Dogs (tibial slope > 20°) • Indications (humans): • pre-osteoarthritis • a large ATT (> 10°) • excessive tibial slope (>13°)
Surgically should aim to adjust sagittal slope according to patient characteristics ACL deficient knee – decrease slope • PCL deficient knee – increase slope • Ligamentous intact knee – maintain slope
Techniques • Lateral closing wedge • Medial opening wedge • Acute opening • Distraction osteogenesis • Dome
Lateral closing wedge – current systems • Accurate cuts • Accurate angle • Predetermined wedge apex • Tight closure • Rigid fixation • More likely to decrease slope
Rx of the Fibula options • Take down tib./fib. joint • Shell out fib. head • Resect at fib. neck • Resect at prox. 1/3
Techniques – Domebest for severe deformities Courtesy D Paley, Principles of Deformity Correction, Springer Verlag, 2002
Opening Wedge/Ext. Fix • Pin placement • Corticotomy • Test distraction • Lock in compression
Opening Wedge/Ext. Fix • Compress x 1 week • Open @ 1 mm/day • Correction + 1.0 mm • Lock • Fix. locked until bony healing (~10-12 wks) • Remove fix. but leave pins-1 wk. • Recheck correction • Remove pins
Advantages of Open Wedge/Ext. Fix • No fibular osteotomy • Small skin incisions • Exact correction of deformity • No change in prox. tibia shape • No added lat. soft tissue lax. • No shortening of limb
Disadvantages of Open Wedge/Ext. Fix • Frame worn medially • Pos. pin tract infection • Pos. joint infection • 2nd procedure to remove • Tightens ext. mech. • Time to healing