Stroke and TIA
Stroke and TIA. Dr. Tallam Prepared by T. Gifford. Stroke – any disease process that interrupts blood flow to the brain Ischemic – 80% Hemorrhage – 20%. Definitions. Thrombotic Most common Atherosclerosis Vasculitis Dissection Polycythemia Hypercoagulable

Stroke and TIA
E N D
Presentation Transcript
Stroke and TIA Dr. Tallam Prepared by T. Gifford
Stroke – any disease process that interrupts blood flow to the brain Ischemic – 80% Hemorrhage – 20% Definitions
Thrombotic Most common Atherosclerosis Vasculitis Dissection Polycythemia Hypercoagulable Develop over minutes to hours Often previous TIA in same distribution Embolic Intravascular material is released occluding vessel downstream No underlying vascular disease at site Valvular vegetations Mural thrombi Cardiac tumors Fat embolism Drug injection Ischemic Stroke
Hypoperfusion Usually from cardiac failure Less common Symptoms wax and wane as blood pressure changes. Ischemic Stroke
Hemorrhagic Stroke • Types • Intracranial hemorrhage (ICH) • Bleeding directly into parenchyma from weakened small arterioles • Non traumatic subarachnoid (SAH) • Blood leaks from cerebral vessel into subarachnoid space • Berry aneurysm rupture
History HTN CAD DM A-fib Valve repair Recent MI Recent TIA Clinical
Febrile – R/O infection Skin Janeway lesions Osler nodes Bleeding dyscrasias Cardio/Lungs Rales S3 Carotid bruit Physical Exam
Fundoscopic exam Papilledema Mass lesion Cerebral vein thrombosis HTN crisis Pre-retinal hemorrhage SAH Physical Exam
Goal Localize CNS lesion NIH Scale Neurological Exam
Level of consciousness Visual assessment Motor function Cerebellar function Sensation and neglect Language Cranial nerves Neurological Exam
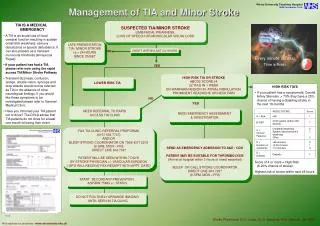
TIA Neurological deficit that resolves within 24 hours (some say 30min) Stroke Syndromes
Anterior cerebral artery infarction Contralateral leg weakness greater than arm weakness Mild cortical sensory deficits Ischemic Stroke Syndromes
Middle cerebral artery infarction Contrlateral weakness and numbness Variably affecting the face and arm greater than leg If dominant hemisphere – aphasia often present Neglect / inattention – non dominant hemisphere Homonymous hemianopsia / gaze toward infarct common Ischemic Stroke Syndromes
Ischemic Stroke Syndromes • Posterior cerebral artery infarction • May be unaware of symptoms • Minimal motor involvement • Light touch / pin prick reduced • Vertibrobasilar syndrome • Posterior circulation compromised • Crossed neurological defecits • Ipsilateral CN deficit, contralateral motor weakness • Dizziness, vertigo, diploplia • Wallenberg syndrome • Ipsilateral loss facial pain and temp with contralateral in body
Ischemic Stroke Syndromes • Basilar artery syndrome • Quadraplegia • Coma • Locked in syndrome • Lesion in pontine tectum with complete muscle paralysis with exception of upward gaze • Cerebellar infarction • “drop attack”, vertigo, H/A, N/V, neck pain • After 6-12 hours cerebral edema develops • MRI / MRA – surgical decompression
Ischemic Stroke Syndromes • Lacunar infarct • Pure motor or sensory deficits caused by infarct of small penetrating arteries • Associated with chronic hypertension • Primarily in pons and basal ganglia • Arterial dissection • Associated with trauma / turning of head or spontaneously • Hypertension is risk factor • Severe neck pain, H/A hours to days before symptoms
Hemorrhagic StrokeSyndromes • ICH • Clinically indistinguishable from infarction • H/A, N/V proceed deficit. • Cerebellar hemorrhage • Sudden onset dizziness, vomiting, truncal ataxia, inability to walk • May be associated with gaze palsy and stupor
SAH Severe constant H/A often in occipital or nuchal area Vomiting common, decrease LOC Sentinal hemorrhage Sudden presentation Hemorrhagic Stroke Syndromes
Diagnosis • Education • Patients (911 usage) • EMS – careful ID of onset if possible • Triage • Antithrombolysis screening
Diagnosis • Tests • Emergent non contrast CT • Ischemic strokes need at least 6 hours before visibility • Identifies all parenchymal bleeds >1cm and 95% of SAH (if done within 12 hours) • Lumbar puncture • If high suspicion of SAH persists after CT • EKG • Identify a-fib or AMI • Labs • MRI / MRA • Carotid ultrasound
Epidural / Subdural Hyponatremia Postictal paralysis (Todd) HTN encephalopathy Brain tumor / Abscess Meningitis / encephalitis Hyperosmotic coma Wernicke encephalopathy Labyrinthitis Drug toxicity Bell palsy Complicated migraine Meniere disease Demyelinating disease Differentials
General ABC’s, O2, Monitor HOB elevated Cardiac monitor IV access Judicious fluids Refrain from glucose containing fluids (no evidence to support) Seizures Treat seizure with ativan and load with fosphenytoin. No prophylaxis Treatment
Hypertension Consider persistent elevation >220 systolic for treatment Use easily titratable meds Lebatelol Enalaprit NTG paste May need to treat to qualify for tPA Treatment
NINDS study Milticenter, randomized, double-blind, placebo 624 patients At 3 months, rtPA group was 30% more likely to have minimal or no disability Symptomatic ICH 6.4% compared to 0.6% Other studies have had variable results FDA approved for ischemic stroke in 1996 Supported by AHA AAN ACEP Thrombolysis
Pre Screen tPa Dose 0.9mg/kg, max 90 mg 10% as bolus Remainder over 60 min No ASA or Heparin in 24 hours after administration Thrombolysis
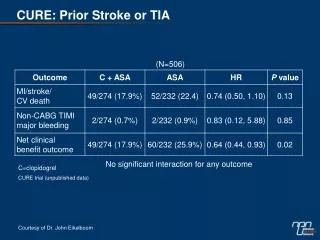
Treatment in tPA Non-Candidates • Goal of secondary stroke prevention • Antiplatelets • ASA 50-300mg daily • Reduced risk by 20-25% • Dipyridamole 200 mg BID • Reduced risk by 15% alone • Dipyridamole + ASA • Reduced risk by 37% • Plavix 75 mg daily • Marginally superior to ASA
Treatment in tPA Non-Candidates • Goal of secondary stroke prevention • Anticoagulants • UFH – efficacy lacking, possible harmful • Increased rate ICH • Decreased rate recurrent ischemic stroke • The use of UFH, LMWH or heparinoids is therefore not recommended for stroke or TIA treatment based on current evidence • Warfarin is indicated for those with A-fib and TIA
Cerebellar infarction Early neurosurgical consultation TIA New onset Admit for evaluation of sources of emboli or stenosis Some recommend UFH when: Known high grade stenosis Cardioembolic source (except infective endocarditis) Crescendo TIAs TIAs despite antiplatelets Early carotid endarterectomy if >70% stenosis Treatment
ICH Treat severe hypertension SBP >220 DBP >120 Slow reduction unless cardiac failure or dissection Elevate HOB 30 degrees Increased ICP Hyperventilation Paco2 target 30-35 Osmotherapy Mannitol 1.0 g/kg IV Target <=310 mOsm/kg Lasix 10 mg IV Consider seizure prophylaxis Surgical consultation Treatment
SAH Rebleed and vasospasm are major complications Keep SBP < 160 Nimodipine 60 mg q 6 hr Reduces incidence and severity of vasospasm Prophylactic phenytoin Antiemetics Surgical consultation Treatment