Download
1 / 20
230 likes | 422 Views
Proposed Medical Staff Re-organization. Medical Staff Meeting June 25, 2008. Purpose of the Medical Staff Organization. Assuring Quality Care For All Patients. Assuring Quality Care through. Effective Self Governance Advising the Hospital on matters affecting quality.

E N D
Proposed Medical Staff Re-organization Medical Staff Meeting June 25, 2008
Purpose of the Medical Staff Organization Assuring Quality Care For All Patients
Assuring Quality Care through . . • Effective Self Governance • Advising the Hospital on matters affecting quality.
Issues Raised by Medical Staff • Meetings are dominated by “dog and pony” shows; not physician driven. • Many meetings are poorly attended / not effective. • Effective Meetings = Specialty- or Issue-specific. • Too long to move an issue through the current structure. • High potential to lose track of an issue. • Many opportunities for change involve more than one specialty to address. To continue Medical Staff influence in the hospital, we need a structure that is more effective in decision-making.
Rebuilding an Influential Medical Staff COMMUNICATION PEER REVIEW LEADERSHIP DEVELOPMENT MEDICAL STAFF FUNCTION & FORM (i.e. Organization) COMMUNICATION
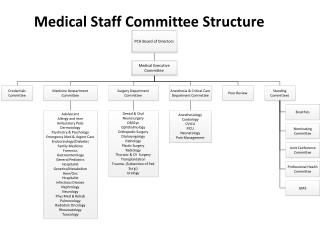
Conceptual Design Board of Directors (Joint Commission Required) Bylaws/Credentials Committee Medical Executive Committee (Joint Commission Required QRC DIVISIONS of the MEDICAL STAFF Hospital Based Surgeons & Interventionalists Medicine Community Medicine SPECIALTIES OF THE MEDICAL STAFF
Conceptual Design DIVISIONS of the MEDICAL STAFF Community Medicine Est. 56 Hospital Based Est. 48 Surg & Intervent. Est. 76 Medicine Est. 61 SPECIALTIES of the MEDICAL STAFF Dentists Anesth Emerg OMS FamMed Card FamMed Gastro Allergy Hospitalists OB/GYN Pulm/CC MedOnc Derm GenSurg Endocrin Path Neo PMR IM ID Ortho Psych NeuroSurg Rheum Neuro Neph ENT Radiology Pod Ophth Plastic Peds Rad Onc Thoracic IM Urology Pain Med Ophth Card
Feedback • Support for trying something new. • Appreciation for flexibility and less formality. • Requests to better understand how issues are managed and resolved in this proposed structure. • Request for assurance that Voice by Specialty or by Individual could be lost. • Why does Community Medicine division have as much representation on MEC as divisions with greater hospital involvement?
Changes Made Include • Changes made to Division leadership roles. • Changes made to MEC membership. • Changed division assignments to “by President with member input”. • Changed Division name to “Surgeons and Interventionalists” • Stressed that any combination of Specialties can meet as desired. • Stressed that one goal is elimination of formality – Meet wherever and whenever and report in. • Clarified that the activity is focused on Specialties. • Divisions meet as needed. • Elected Division Leadership serve as facilitators and communicators. • Clarified that Provider Support Services will continue to coordinate and document as needed.
Medical Executive Committee • Voting members include: • President, President-Elect, and Secretary-Treasurer • Division Chief from all 4 Divisions • Vice Chief from Hospital-Based, Surgeons & Interventionalists, and Medicine Divisions • Total of 10
Medical Executive Committee • Business includes: • Performing the required regulatory duties of the medical staff; • Acting on the recommendations coming up through the structure; • Resolving issues only if they cannot be otherwise resolved. • Ensuring effective and efficient decision-making leading to continued medical staff influence in the hospital.
Division Leadership:Division members elect Chief, Vice Chief, & Member at Large • Chief , Vice Chief & Member at Large cannot be from same specialty within a Division • Chief and Vice Chief serve on MEC (Chief only from Community Medicine) • Member at Large responsible for overseeing peer review for Division and serves on QRC • Vice Chief responsible for overseeing credentialing and serves on Bylaws/Credentials.
DIVISIONS: Coordination & Collaboration • Responsible for consulting specialties and members of • each division for patient care initiatives, problem • solving, etc. • Collaboration As Needed. Attend meetings as interested. • Drawn together by like types of care and how • practitioners work together to provide that care. • Shared interests, reflecting many existing cross- • specialty activities. DIVISIONS of the MEDICAL STAFF Hospital Based Surgs/Intervents Medicine Community Med SPECIALTIES
SPECIALTIES: Freedom & Flexibility • Grassroots Structure • Identifies and Drives Issues up through the Structure • Flexible; Avoid Regulatory Requirements • Physician-Driven Agendas • Meet when/how/where/for what; no required content or • minutes • Meet in any combination with other Specialties as desired. • Utilize any type of communication to conduct business • PSS always available to coordinate, document, etc. • Each Specialty elects a Representative SPECIALTIES
Specialty’s Voice • More even balance between Divisions; More opportunity for all specialties to participate. • Free to address own affairs w/o regulatory constraints. • Multiple ways for members to participate (meetings, blogs, emails, faxes). • Accountability to participate if want to have influence. • Responsibility to Trust elected Leaders & support decisions.
Individual Voice Any medical staff member may: • Contact any medical staff leader to voice a concern; • Contact any medical staff officer to elevate a concern. • Attend MEC to elevate a concern. • Any medical staff member may attend at the invitation of their Division Chief attend MEC to voice a concern and vote on that matter. • Participate regularly and timely in providing input into recommendations as they are considered via multiple channels (meetings, blogs, email, ballots) • Vote on matters within Specialty, Division and Medical Staff as a Whole. • Even after policy decisions are made, a petition process for reconsideration exists.
Form Follows FunctionHow do we want to function? • Empower Physician Driven Agendas • Technology to give us options other than meetings, when appropriate • Right People – Right Place – Right Time • Remove regulatory-induced formality • Work effectively despite % of medical staff disinterested or too busy • Empowered core of leadership to ensure efficient decision-making and continued influence in the hospital
Two Way Communication • Leadership is accountable to ensure information is in weekly or special newsletters and on electronic bulletin board. Future: Interactive Website • Leadership is accountable to adequately notify constituents using technology or traditional methods regarding issues & opportunities. • Members are accountable to receive information using these focused sources to stay informed. • Members are accountable to provide input in a timely manner.
Patients count on the Medical Staff to counsel the Hospital effectively regarding things that impact Quality of Care. In order to promote the influence of the Medical Staff with the Board and Administration, the Medical Staff must function effectively.
Where do we go from here? • Is this structure perfect? No • Is it an individualized model similar to that working for other medical staffs? Yes • Is it a well-thought out alternative with a high probability of success?Yes • Will we modify it over time as we learn? Yes Please Vote YES