Download
1 / 10
160 likes | 793 Views
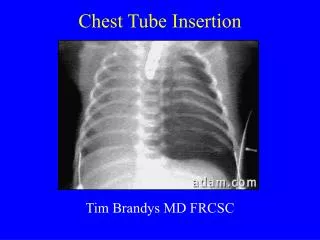
Chest tube insertion lab. Tube placement sites. Depends on purpose Anterior (triangle of safety) Pneumothorax Low lateral (Ultrasound guidance really helps) Fluid drainiage. Indications. Triangle of Safety. Incision and Insertion Sites. Dissection OVER rib. Chest tube size. Air: small

E N D
Tube placement sites • Depends on purpose • Anterior (triangle of safety) • Pneumothorax • Low lateral (Ultrasound guidance really helps) • Fluid drainiage
Chest tube size • Air: small • Fluid: medium • Blood: Large • Pus: Large
Alternate procedures • Simple needle aspiration and recheck • For simple pneumothorax only: • Small • No tension • Underwater seal jar • Heimlich valve
Tube removal criteria • Pneumothorax: no bubbling and lung expanded • Consider an interval of tube clamping before removal • Probably best to not remove while on mechanical ventilation, especially with PEEP • Drainage: less than 200 cc/24 hours • Take care to seal hole during and after removal! • Follow-up chest x-ray
Complications • Bleeding and hemothorax due to intercostal artery perforation • Perforation of visceral organs (lung, heart, diaphragm, or intra-abdominal organs) • Perforation of major vascular structures such as the aorta or subclavianvessels • Intercostal neuralgia due to trauma of neurovascular bundles, • Subcutaneous emphysema, • Re-expansion pulmonary edema • Infection of the drainage site • Pneumonia, and empyema • Technical problems such as intermittent tube blockage from clotted blood, pus, or debris, or incorrect positioning of the tube, which causes ineffective drainage.