
Please Read First
E N D
Presentation Transcript
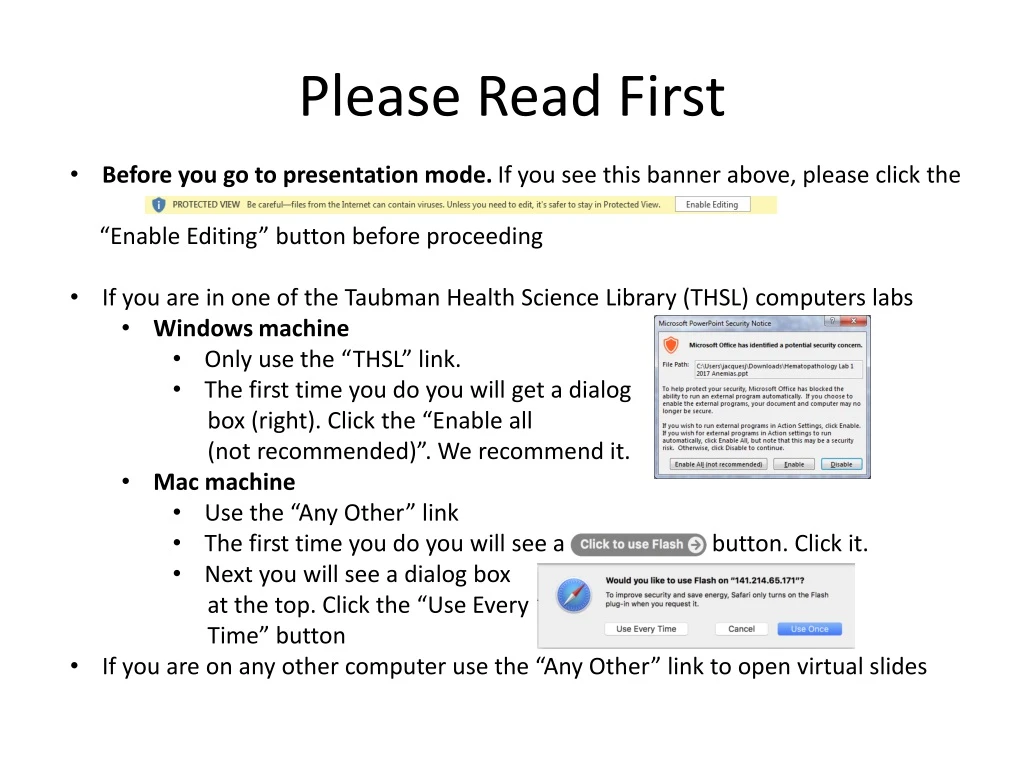
Please Read First • Before you go to presentation mode. If you see this banner above, please click the • “Enable Editing” button before proceeding • If you are in one of the Taubman Health Science Library (THSL) computers labs • Windows machine • Only use the “THSL” link. • The first time you do you will get a dialog • box (right). Click the “Enable all • (not recommended)”. We recommend it. • Mac machine • Use the “Any Other” link • The first time you do you will see a button. Click it. • Next you will see a dialog box • at the top. Click the “Use Every • Time” button • If you are on any other computer use the “Any Other” link to open virtual slides
Work through the slides, questions, answers and virtual slides using the PowerPoint show (PPS). The micrographs are displayed adjacent to micrographs of a "normal" or "look-alike" abnormal smear at the same magnification. The micrographs should serve as a guide for viewing the virtual slides. The virtual slides can be accessed from links embedded in the PPS (if you are using a workstation or laptop on the Medical School Campus). A “self-test tool” for the virtual slides is available as well. Self-test tool (THSL) Self-test tool (Any Other) Hematopathology Lab 2 Start Slide Show Read history, review image stacks (space bar, arrow, mouse click) Space bar, arrow, mouse click to reveal question Space bar, arrow, mouse click to reveal answers After working through case using PPS, open virtual slide (links in PPS) and review
Normal smears Blood smear stack Bone marrow stack Virtual Slide Normal Blood Smear (Web viewer) Virtual Slide Normal Marrow Smear (Web viewer) (THSL) (Any Other) Virtual Slide Normal Blood Smear (Web viewer) Virtual Slide Normal Marrow Smear (Web viewer)
CASE #1 & #2History #1: 58-year-old male with increasing weakness, fatigue, malaise, unexplained lower extremity bruises and weight loss over the previous six weeks. Petechiae on exam. WBC = 155,000 cells/mm3, Hb = 9.0 gm/dl, platelets = 11,000/mm3. History #2: Four-year-old female with fever, pharyngitis, and otitis, unresponsive to antibiotics. Increasing fatigue, malaise, and nondescript bone and joint pains. Conjunctival pallor and petechiae on her lower extremities. WBC = 55,000 cells/mm3, Hb = 7.6 gm/dl, platelets = 5,000/mm3. History #1 stack History #2 stack (THSL) Virtual Slide History #1 (Web viewer) Virtual Slide History #2 (Web viewer) (Any Other) Virtual Slide History #1 (Web viewer) Virtual Slide History #2 (Web viewer)
CASE #1 & #2History #1: 58-year-old male with increasing weakness, fatigue, malaise, unexplained lower extremity bruises and weight loss over the previous six weeks. Petechiae on exam. WBC = 155,000 cells/mm3, Hb = 9.0 gm/dl, platelets = 11,000/mm3. History #2: Four-year-old female with fever, pharyngitis, and otitis, unresponsive to antibiotics. Increasing fatigue, malaise, and nondescript bone and joint pains. Conjunctival pallor and petechiae on her lower extremities. WBC = 55,000 cells/mm3, Hb = 7.6 gm/dl, platelets = 5,000/mm3. What are the major abnormalities on the smear? Many (>20%) of the leukocytes are large mononuclear cells with nuclei containing lighter-staining, finely-textured chromatin and occasional nucleoli (some multiple). These fit the general category of "blast" forms. In addition to the markedly elevated white cell counts (with a predominance of blasts), the patients are anemic and profoundly thrombocytopenic. Are these two histories and smears from patients with acute leukemias, viral infections or sepsis ? Acute leukemias. It can be difficult for the novice to distinguish a reactive lymphocytosis (e.g., in florid infectious mononucleosis) from leukemia based on the appearance of the atypical cells in the smear alone. The history, CBC and clinical findings are crucial pieces of information. Patients with acute leukemia have signs, symptoms and laboratory findings indicating bone marrow insufficiency or failure in addition to the presence of blast forms. Patients with reactive lymphocytosis generally do not have such findings.
CASE #1 & #2History #1: 58-year-old male with increasing weakness, fatigue, malaise, unexplained lower extremity bruises and weight loss over the previous six weeks. Petechiae on exam. WBC = 155,000 cells/mm3, Hb = 9.0 gm/dl, platelets = 11,000/mm3. History #2: Four-year-old female with fever, pharyngitis, and otitis, unresponsive to antibiotics. Increasing fatigue, malaise, and nondescript bone and joint pains. Conjunctival pallor and petechiae on her lower extremities. WBC = 55,000 cells/mm3, Hb = 7.6 gm/dl, platelets = 5,000/mm3. Look carefully at multiple abnormal cells. Does their appearance provide any clues that help refine the diagnosis? Case history #1: Some blasts have cytoplasmic granularity and a few have needle-shaped cytoplasmic inclusions (Auer rods). Case history #2: Blasts have a high nuclear/cytoplasmic ratio and agranular cytoplasm. What are the most likely diagnoses based on smear findings? Acute leukemias (blast percentage in both greater than 20%). Case History #1: Acute Myeloid Leukemia (AML). The presence of some Auer rods in this case establishes the diagnosis of AML and excludes the possibility of acute lymphoblastic leukemia (ALL). Additional laboratory testing is still needed for precise subclassification of the AML according to WHO guidelines and for risk stratification (see below). Case History #2: Most likely an Acute Lymphoblastic Leukemia (ALL) but additional studies always needed for confirmation since minimally differentiated AML can have a similar appearance. Also must separate B lymphoblastic and T lymphoblastic subtypes for prognostic/therapeutic purposes (see below). Lymphoblastic neoplasms may present as “leukemias” (bone marrow and blood involvement primarily), or “lymphomas”, (thymic, nodal, or extranodal infiltrates primarily). Name reflects this behavior: B lymphoblastic or T lymphoblastic leukemia/lymphoma. Frequencies vary in children and adults (ALL > AML in children; AML > ALL in adults). Clinical presentations and approach to diagnosis similar, regardless of age. Is a bone marrow aspirate and biopsy necessary to establish the diagnosis? Sometimes. If the blast percentage in the peripheral blood equals or exceeds 20%, then the diagnosis of acute leukemia is established. If the blast percentage in the peripheral blood is <20%, then a bone marrow aspirate and biopsy are generally required for diagnosis since other stem cell neoplasms may also result in circulating blasts (e.g., some myelodysplastic syndromes and chronic myeloproliferative neoplasms). Can flow cytometry help with the diagnosis? Absolutely. Confirms lineage (i.e., AML vs. ALL). Subtypes ALL (i.e., B lymphoblastic or T lymphoblastic). Use panel of antibodies that react with stem cell, granulocytic, monocytic, T and B cell antigens. Routinely part of the initial diagnostic work-up for acute leukemias.
CASE #1 & #2History #1: 58-year-old male with increasing weakness, fatigue, malaise, unexplained lower extremity bruises and weight loss over the previous six weeks. Petechiae on exam. WBC = 155,000 cells/mm3, Hb = 9.0 gm/dl, platelets = 11,000/mm3. History #2: Four-year-old female with fever, pharyngitis, and otitis, unresponsive to antibiotics. Increasing fatigue, malaise, and nondescript bone and joint pains. Conjunctival pallor and petechiae on her lower extremities. WBC = 55,000 cells/mm3, Hb = 7.6 gm/dl, platelets = 5,000/mm3. What additional information is needed for precise classification, risk stratification and treatment decisions ? The current classification of acute leukemias was developed by an international panel under the auspices of the World Health Organization (WHO) and published in 2008. The WHO guidelines emphasize cytogenetic (karyotypic) and molecular features (e.g., mutations in NPM1, CEBPA, FLT3) in conjunction with morphologic, immunophenotypic (flow cytometric), and clinical characteristics (antecedent history of cytotoxic therapy?; antecedent history of a myelodysplastic syndrome?). The importance of molecular genetic testing will grow as more genetic lesions and corresponding targeted therapies are discovered. Accurate lineage assignment is important because treatments for acute myeloid leukemia (AML) and acute lymphoblastic leukemia (ALL) are different. Also some “recurrent genetic abnormalities” determine treatment choice (e.g., all-trans retinoic acid (ATRA) or arsenic trioxide for acute promyelocytic leukemia, t(15;17)(PML-RARA); tyrosine kinase inhibitors for B lymphoblastic leukemia with Philadelphia chromosome, t(9;22)(BCR-ABL)). Genetic features linked to risk of progression, risk of relapse, and/or resistance to available chemotherapies contribute to “risk stratification” and treatment choice as well.
CASE #3: 55-year-old female presents with increasing fatigue, night sweats, weight loss, and abdominal "fullness." The patient has marked splenomegaly, 10 cm below the left costal margin, without lymphadenopathy. The CBC showed: WBC = 105,000 cells/mm3, Hb = 10.5 gm/dl, and platelets = 85,000/mm3. Normal smear stack Patient stack (THSL) Virtual Slide Normal Blood Smear (Web viewer) Virtual Slide Patient Blood Smear (Web viewer) (Any Other) Virtual Slide Normal Blood Smear (Web viewer) Virtual Slide Patient Blood Smear (Web viewer)
CASE #3: 55-year-old female presents with increasing fatigue, night sweats, weight loss, and abdominal "fullness." The patient has marked splenomegaly, 10 cm below the left costal margin, without lymphadenopathy. The CBC showed: WBC = 105,000 cells/mm3, Hb = 10.5 gm/dl, and platelets = 85,000/mm3. What are the major abnormalities on the smear? Marked neutrophilia with full spectrum of granulocytic maturation evident. Prominent granulocytic left shift includes precursors normally found in the bone marrow (see virtual slide of normal bone marrow for comparison: Virtual Slide Normal Marrow Smear-”THSL” ; Virtual Slide Normal Marrow Smear-”Any Other” ). Overall percentage of precursors higher than usual reactive left shift (this leukocyte differential features a “myelocyte bulge”, and percentage of blasts is not substantially increased). Basophils are also notably increased (more than in a typical reactive leukocytosis). What is the differential diagnosis based on the CBC and blood smear? Chronic myelogenous leukemia (CML), chronic phase versus a leukemoid reaction (marked reactive leukocytosis). Would flow cytometry help with the diagnosis? No. We know from the morphology that this is a myeloproliferative process with normal-appearing granulocytes and precursors. There are no antigenic findings that can separate chronic phase CML from a reactive leukocytosis. When might flow cytometry be useful in the context of a “chronic” myeloproliferative disorder ? Would cytogenetic or molecular genetic tests help with the diagnosis? Absolutely, since the acquired structural genetic defect that causes CML has been identified. The Philadelphia chromosome t(9;22) can be detected in the neoplastic cells using cytogenetic karyotyping. The translocation creates the chimeric fusion gene BCR-ABL, and it can also be detected using molecular diagnostic techniques such as reverse transcriptase polymerase chain reaction (RT-PCR) or fluorescence in situ hybridization (FISH). Demonstration of either the Philadelphia chromosome or the BCR-ABL fusion is required for diagnosis.
CASE #3: 55-year-old female presents with increasing fatigue, night sweats, weight loss, and abdominal "fullness." The patient has marked splenomegaly, 10 cm below the left costal margin, without lymphadenopathy. The CBC showed: WBC = 105,000 cells/mm3, Hb = 10.5 gm/dl, and platelets = 85,000/mm3. What is the natural course of this disease? How does one monitor progression? The BCR-ABL gene fusion (formed by t(9;22)) encodes a chimeric fusion protein with a constitutively active tyrosine kinase domain that affects many downstream signaling cascades. Clonal expansion and immortalization of the pluripotential hematopoietic stem cell occurs. In the chronic phase of the disease (lasting several years, on average, in untreated individuals), the daughter cells of the leukemic stem cells continue differentiating primarily down the granulocytic lineage. The bone marrow fills up with normal looking granulocytic precursors that spill out into the bloodstream and also accumulate in extramedullary sites such as the spleen. Over time, additional chromosomal aberrations and genetic mutations accumulate that impair the ability of affected cells to mature and differentiate; this results in an increased percentage of blasts in the neoplastic population. When the percentage of blast forms in the blood or bone marrow of a CML patient is > 10% but < 20%, then the patient is considered to be in an "accelerated phase” of the disease. When the percentage of blast forms in the blood or bone marrow reaches 20% or greater, then the patient is deemed to be in the “blast phase” of the disease; this is morphologically indistinguishable from acute leukemia. In about two-thirds of cases of blast progression of CML the blasts will have a myeloid immunophenotype, and the remainder will have a lymphoid immunophenotype; this dichotomy reflects the stem cell nature of the neoplasm. Treatment of blast phase CML depends, in part, on the lineage of the blasts (myeloid vs. lymphoid). It is often impossible to determine lineage based solely on microscopic appearance of the blasts. Ancillary tests such as flow cytometric immunophenotyping (detects lineage-specific antigens on cell surface or in cytoplasm) and cytochemical stains (detect enzymes associated with “myeloid” differentiation) can make this determination.
SUPPLEMENTAL CASE A (for comparison to CASE #3): After a several day prodrome of fever, chills, cough, and shortness of breath, an elderly patient presented to the emergency department (ED). In the ED, the subject was febrile, hypotensive and hypoxemic. The white count was elevated. Normal smear stack Patient stack Virtual Slide Normal Blood Smear (Web viewer) Virtual Slide Patient Blood Smear (Web viewer) (THSL) (Any Other) Virtual Slide Normal Blood Smear (Web viewer) Virtual Slide Patient Blood Smear (Web viewer)
SUPPLEMENTAL CASE A (for comparison to CASE #3): After a several day prodrome of fever, chills, cough, and shortness of breath, an elderly patient presented to the emergency department (ED). In the ED, the subject was febrile, hypotensive and hypoxemic. The white count was elevated. What are the major WBC abnormalities on the smear? There is a neutrophilic leukocytosis with a “left shift” in the granulocytic series (increased proportion of bands as well as occasional less mature myeloid precursors). The left shift is not as prominent as in Case #3, however, lacking the “myelocyte bulge” characteristic of chronic phase CML. Many of the neutrophils have “toxic” cytoplasmic granulation and occasional Dohle bodies are present; these features favor a reactive neutrophilia rather than a neoplastic one. There is an accompanying thrombocytosis, a frequent finding in reactive/inflammatory states. What additional studies are needed to establish a diagnosis? The history and blood smear findings are strongly suggestive of a serious infectious process and possible sepsis. Sepsis is defined as the presence, or presumed presence, of an infection accompanied by evidence of a systemic response referred to as the "systemic inflammatory response syndrome" (SIRS). Tests aimed at diagnosing infection in organ/tissues (e.g., chest X-ray) and blood (e.g., microbial culture) are always part of the workup. What other conditions might you consider? If elevation in the neutrophil count is marked, sustained, and associated with prominent increases in early granulocytic precursors (e.g. metamyelocytes, myelocytes) and other less frequent leukocyte types (e.g., basophils), and there is no clinical evidence of a precipitating infection/inflammatory disorder, then chronic myeloproliferative neoplasms (e.g., chronic myelogenous leukemia) are considerations. How are the morphologic abnormalities in the blood smear related to the symptoms, signs and complications in this disease? The changes in the blood smear indicate that the bone marrow is responding to a strong inflammatory stimulus (mediated by relevant cytokines and growth factors).
CASE #4: The patient is a healthy 65-year-old male who was noted to have slightly enlarged axillary and cervical lymph nodes on an annual physical examination. The patient offered no complaints and was given a "clean bill of health" one year previously. No organomegaly was noted. The CBC showed: WBC = 45,000 cells/mm3, Hb = 13.5 gm/d., platelets = 185,000/mm3. Compare the blood smear in this patient to the normal and abnormal smears from other cases. Normal smear stack Patient stack (THSL) Virtual Slide Normal Blood Smear (Web viewer) Virtual Slide Patient Blood Smear (Web viewer) (Any Other) Virtual Slide Normal Blood Smear (Web viewer) Virtual Slide Patient Blood Smear (Web viewer)
CASE #4: The patient is a healthy 65-year-old male who was noted to have slightly enlarged axillary and cervical lymph nodes on an annual physical examination. The patient offered no complaints and was given a "clean bill of health" one year previously. No organomegaly was noted. The CBC showed: WBC = 45,000 cells/mm3, Hb = 13.5 gm/d., platelets = 185,000/mm3. Compare the blood smear in this patient to the normal and abnormal smears from other cases. What are the major abnormalities on the smear? Too many small lymphocytes are present (absolute lymphocytosis). The lymphocytes are uniformly small with densely clumped nuclear chromatin (sometimes described as “soccer-ball”, “cracked-mud”, or “ginger-snap” nuclear chromatin appearance), inconspicuous nucleoli, and scant, agranular cytoplasm. What is the differential diagnosis based on the CBC and blood smear? Chronic lymphocytic leukemia (CLL) or leukemic phase of lymphoma (lymphoid neoplasms that arise in any lymphoid organ or other tissue may come to involve the peripheral blood in some instances) versus a reactive lymphocytosis. To resolve this differential diagnosis, one needs a test that can help determine whether the lymphoid cells are primarily monoclonal B-cells, clonally “aberrant” T-cells, or a mixture of polyclonal T-cells and polyclonal B-cells. How may flow cytometry help to establish the diagnosis? (click to see display of flow cytometry dot plots)
CASE #4: The patient is a healthy 65-year-old male who was noted to have slightly enlarged axillary and cervical lymph nodes on an annual physical examination. The patient offered no complaints and was given a "clean bill of health" one year previously. No organomegaly was noted. The CBC showed: WBC = 45,000 cells/mm3, Hb = 13.5 gm/d., platelets = 185,000/mm3. Compare the blood smear in this patient to the normal and abnormal smears from other cases. How did flow cytometry help to establish the diagnosis in this case? Flow cytometric immunophenotyping served to identify and quantify the size of a monoclonal B-cell population in the blood. In this case, the presence of aberrantly expressed antigens (e.g., unusual density of B-cell antigens or the aberrant presence of antigens normally found on other cell types) helped confirm a neoplasm and assisted with proper subclassification of the neoplasm. The low antigen density of CD20, low antigen density of monotypic surface immunoglobulin, aberrant CD5 expression, and CD23 are characteristic of chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL). The flow data in this case show that nearly all of the B lymphocytes express a single light chain type (kappa) on their surfaces; therefore, they are monoclonal. Normally there are many more T-cells than B-cells in the blood, and the B-cells are a balanced mixture of cells expressing kappa or lambda light chains (normal kappa:lambda ratio = 0.5-2:1).
SUPPLEMENTAL CASE B (for comparison to CASES #2 and #4): A 20-year-old man was admitted with a three day history of fever, sore throat, and malaise. He had cervical lymphadenopathy, non-exudative pharyngitis, slight hepatomegaly and splenomegaly (2 cm below the costal margin). He had mild left and right abdominal tenderness without guarding. Normal CBC except for an elevated percentage of lymphocytes (see virtual slide). Normal smear stack Patient stack (THSL) Virtual Slide Normal Blood Smear (Web viewer) Virtual Slide Patient Blood Smear (Web viewer) (Any Other) Virtual Slide Normal Blood Smear (Web viewer) Virtual Slide Patient Blood Smear (Web viewer)
SUPPLEMENTAL CASE B (for comparison to CASES #2 and #4): A 20-year-old man was admitted with a three day history of fever, sore throat, and malaise. He had cervical lymphadenopathy, non-exudative pharyngitis, slight hepatomegaly and splenomegaly (2 cm below the costal margin). He had mild left and right abdominal tenderness without guarding. Normal CBC except for an elevated percentage of lymphocytes (see virtual slide). What are the major WBC abnormalities on the smear ? Increased percentage of large, atypical lymphocytes with abundant, bluish cytoplasm and big nuclei with irregular contours. Cell membranes of the atypical, reactive lymphocytes are often indented by surrounding red blood cells. What additional test(s) are needed to establish a diagnosis? In a young, previously healthy individual without substantial cytopenias on CBC (i.e., no marked anemia, thrombocytopenia or neutropenia), the most likely cause for atypical (reactive) lymphocytes is a viral infection. Infectious mononucleosis is a viral illness commonly associated with lymphadenopathy, splenomegaly, and lymphocytosis with an increased proportion of atypical lymphocytes. Serologic confirmation of the diagnosis is desirable. The “Monospot test" (for heterophile antibody) or other immunoassays for antibodies to Epstein-Barr virus (EBV) are readily available for this purpose. What other conditions should you consider? If Monospot and other EBV serologic tests are negative, then other viral infections are considerations (e.g., cytomegalovirus infection, acute HIV infection). If there was evidence of bone marrow suppression (e.g., neutropenia, anemia, thrombocytopenia) and the atypical lymphocytes were more blastic in appearance, then acute lymphoblastic leukemia (see Case #2) might be a consideration in the differential diagnosis. In contrast to chronic lymphocytic leukemia (CLL; see Case #4), most reactive lymphocytoses feature more cell-to-cell heterogeneity (in size, nuclear shape, visibility of nucleoli, etc). The cytologic homogeneity of the lymphocytes noted in most cases of CLL is a reflection of the monoclonality of that neoplastic process. How are the morphologic abnormalities in the blood smear related to the symptoms, signs and complications in this disease? The atypical lymphocytes in the peripheral blood are predominantly cytotoxic T-cells responding to the EBV-infected B-cells. Some EBV-infected B-cells are in the circulation as well as in lymphoid tissues (e.g., lymph nodes, tonsils, spleen), but these are typically outnumbered by the reactive T-cells. Lymphadenopathy and splenomegaly reflects the proliferative immune response trying to clear infected cells. Splenic rupture is an uncommon complication of infectious mononucleosis.