Download
1 / 34
350 likes | 504 Views
Learn recognition and management of obstetric emergencies like prolapsed cord, shoulder dystocia, and breech delivery to enhance competence in necessary skills.

E N D
Obstetric emergencies Prolapsed cord Shoulder dystocia Breech delivery Twin delivery
Aims • To recognise the above emergencies • To practise the skills needed to manage them • To achieve competence in those skills
Prolapsed cord • The umbilical cord is felt at the vagina following rupture of the membranes or is felt on vaginal examination to be coming down below the presenting part
Prolapsed cord • Look at or gently feel the cord to check if there are pulsations – if pulsating the fetus is alive • Determine the lie and the presenting part; baby may be in transverse lie and if so the mother requires caesarean section • Perform VE to determine the status of the labour
If cord pulsating and first stage of labour… • Stop presenting part pressing on cord • Knee-elbow position • Manually displace the presenting part • Fill the bladder and clamp the catheter • Do not wrap the cord in warm towel • Refer for CS • Consider tocolytics • salbutamol 0.2 mg iv slowly over 2 minutes
If cord pulsating and second stage of labour… • Expedite delivery with episiotomy and vacuum extraction (or forceps) • If the baby is breech, perform a breech extraction • Prepare to resuscitate the newborn
If cord not pulsating… • If the cord is not pulsating the fetus is dead • If fetus is pre-viable or grossly abnormal deliver in manner safest for mother
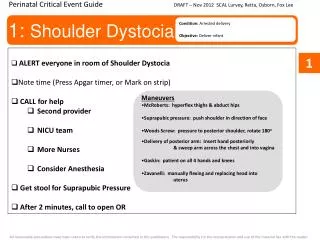
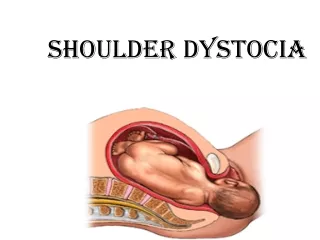
Shoulder dystocia • Not predictable • Fetal head delivered but shoulders stuck behind symphysis pubis • Suspect if; • Unable to deliver shoulder • Fetal head delivered but remains tightly applied to the vulva • Chin retracts and depresses the perineum • Traction on the head fails to deliver the shoulder (should we not delete this last statement?)
Shoulder dystocia • Call for help • McRobert’s • Position knees as far as possible up to the chest and abduct and rotate legs outwards
Shoulder dystocia • Apply suprapubic pressure using the heel of the hands • This should be done from directly above the patient, not from the left or the right of the patient
Shoulder dystocia • Make adequate episiotomy to reduce soft tissue obstruction and make room for other manoeuvres • Apply firm continuous traction on the fetal head but do not pull or tug the neck (Should this not read apply firm downward pressure on the head?)
Shoulder dystocia • Apply pressure to the anterior shoulder in the direction of the baby’s chest, to rotate the shoulder and decrease the inter-shoulder diameter OR • Apply pressure to the posterior shoulder in the direction of the sternum
Shoulder dystocia Try to deliver posterior shoulder first: • grasping the humerus of the posterior arm keeping the arm flexed at the elbow, • sweep the arm across the chest- this will provide room for the anterior shoulder to move under the symphysis
Shoulder dystocia • Keep McRoberts throughout even when moving on to other manoeuvres • If all the above fails then consider fracturing the clavicle
Breech • May be diagnosed at abdominal examination or on vaginal examination during delivery • For vaginal delivery to be possible • The breech must be frank or complete • Pelvis must be adequate • Must not have had previous CS for CPD • Fetus must not be too large (< 3.5kg)
Breech • Allow delivery to proceed until fetal buttocks visible • ‘Hands off’ • As perineum distends decide whether episiotomy necessary and perform • Allow buttocks to deliver until back and then shoulder blades are seen • DO NOT INTERFERE!
Breech • Gently take hold baby around bony pelvis but do not pull
Breech • If legs do not deliver spontaneously, deliver one leg at a time
Breech • Allow arms to disengage spontaneously one by one • Hold newborn by hips (Bony structures!) • Do not pull • Ask mother to push with contractions • After delivery of first arm lift buttocks towards mother’s abdomen to allow second arm to deliver
Breech • If arm does not deliver spontaneously, place one or two fingers in the elbow and bend the arm bringing hand down over face
Breech • If arms stretched above the head or folded around the neck use Lovset’s manoeuvre • Hold newborn by hips and turn half circle keeping the back uppermost • Apply downward traction so posterior arm becomes anterior and deliver arm under pubic arch • Draw arm over chest as elbow is flexed • Deliver second arm by turning back half a circle, back uppermost and applying downward traction
Breech • If body cannot be turned to deliver anterior arm then deliver posterior arm • Hold and lift newborn by ankles • Move newborn’s chest towards mother’s inner leg to deliver posterior shoulder • Deliver the arm and the hand • Lay newborn down by the ankles to deliver anterior shoulder • Deliver arm and hand
Delivery of the head • Allow baby to hang from the perineum until hair line is seen • ONLY prevent baby from dropping off • This allows gradual decent and engagement of the head (moulding has not taken place like in the cephalic presentation, so this process may be slow
Breech Mauriceau-Smellie-Veit • Hold newborn’s body over your hand and arm • Place first and third fingers on newborn’s cheek bones • Use other hand to grasp newborn’s shoulders • With two fingers of this hand flex the newborn’s head towards chest
Breech • Raise the newborn, still astride the arm until the mouth and nose are free
Breech For the stuck head • Apply firm pressure above mother’s pubic bone and push head through pelvis • Consider symphysiotomy
Twin delivery • Can be discovered: • routine abdominal palpation, • during ultrasound or • after delivery of the first baby • Abdominal palpation or VE
Twin delivery- first baby • Start iv infusion • Check presentation • If vertex allow labour to progress as for single vertex • If transverse lie or breech deliver by CS • After the delivery of the 1st baby leave a clamp on the maternal end of the cord and do not attempt to deliver the placenta until the 2nd baby is delivered
Twin delivery- second baby • Check FH • Check IV is running, may be needed for augmentation if contractions are not adequate, may also be needed to manage/prevent PPH • Palpate abdomen to determine lie of second baby • Perform VE to determine • If cord has prolapsed • Whether membranes are intact • Confirm presentation • Correct to longitudinal lie by external version if possible-intact membranes
Twin delivery – second baby • For vertex • Rupture membranes if intact • Check FH between contractions • Anticipate spontaneous delivery • Augment labour if necessary • Vaginal delivery as normal
Twin delivery- second baby • For breech • If contractions inadequate augment • If membranes intact and breech has descended, rupture membranes • Check FH between contractions • Assisted vaginal delivery • Breech extraction if membranes rupture during vaginal examination • If vaginal delivery not possible deliver by C/S
RECAP • Recognition and management of Obstetric emergencies: • Cord prolapse • Shoulder dystocia • Twin delivery • Skills in providing assisted deliveries